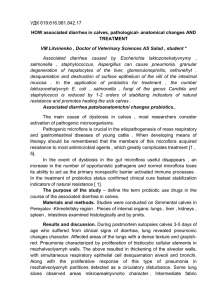
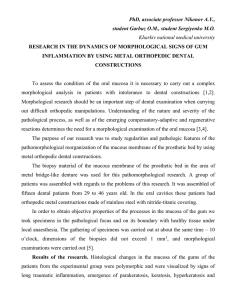
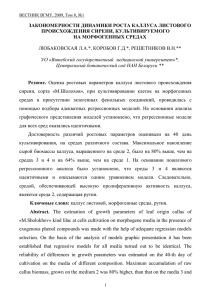
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/6551266 Tissue-engineered Oral Mucosa: a Review of the Scientific Literature Article in Journal of Dental Research · March 2007 DOI: 10.1177/154405910708600203 · Source: PubMed CITATIONS READS 187 6,040 5 authors, including: Keyvan Moharamzadeh Ian m Brook Mohammed Bin Rashid University of Medicine and Health Sciences The University of Sheffield 152 PUBLICATIONS 3,033 CITATIONS 167 PUBLICATIONS 3,905 CITATIONS SEE PROFILE SEE PROFILE Richard van Noort Andy Scutt The University of Sheffield Swansea University 254 PUBLICATIONS 10,283 CITATIONS 110 PUBLICATIONS 6,798 CITATIONS SEE PROFILE All content following this page was uploaded by Andy Scutt on 24 December 2013. The user has requested enhancement of the downloaded file. SEE PROFILE Journal of Dental Research http://jdr.sagepub.com/ Tissue-engineered Oral Mucosa: a Review of the Scientific Literature K. Moharamzadeh, I.M. Brook, R. Van Noort, A.M. Scutt and M.H. Thornhill J DENT RES 2007 86: 115 DOI: 10.1177/154405910708600203 The online version of this article can be found at: http://jdr.sagepub.com/content/86/2/115 Published by: http://www.sagepublications.com On behalf of: International and American Associations for Dental Research Additional services and information for Journal of Dental Research can be found at: Email Alerts: http://jdr.sagepub.com/cgi/alerts Subscriptions: http://jdr.sagepub.com/subscriptions Reprints: http://www.sagepub.com/journalsReprints.nav Permissions: http://www.sagepub.com/journalsPermissions.nav Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research CRITICAL REVIEWS IN ORAL BIOLOGY & MEDICINE Tissue-engineered Oral Mucosa: a Review of the Scientific Literature K. Moharamzadeh1*, I.M. Brook1, R. Van Noort1, A.M. Scutt2, and M.H. Thornhill1 1School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield, S10 2TA, United Kingdom; and 2Department of Engineering Materials, University of Sheffield, Broad Lane, Sheffield, S3 7HQ, United Kingdom; *corresponding author, k.moharamzadeh@sheffield.ac.uk J Dent Res 86(2):115-124, 2007 ABSTRACT Tissue-engineered oral mucosal equivalents have been developed for clinical applications and also for in vitro studies of biocompatibility, mucosal irritation, disease, and other basic oral biology phenomena. This paper reviews different tissue-engineering strategies used for the production of human oral mucosal equivalents, their relative advantages and drawbacks, and their applications. Techniques used for skin tissue engineering that may possibly be used for in vitro reconstruction of human oral mucosa are also discussed. KEY WORDS: oral mucosa, tissue engineering, scaffold, keratinocyte. (I) INTRODUCTION utologous grafts taken from a different part of the oral cavity— A such as free gingival grafts, buccal mucosal grafts, and palatal grafts—are commonly used approaches for repairing soft-tissue defects. Since the cells are taken from the same person, the body does not reject these grafts. However, there are several problems associated with autologous grafts, including: donor site morbidity, tissue shortage, and retention of the original characteristics of the donor tissue. To overcome these problems, in the early 1980s, investigators introduced cultured epithelial sheets of human skin and oral mucosa, from a small biopsy, for the treatment of burns (Madden et al., 1986), and intra-oral grafting (Lauer et al., 1991; Ueda et al., 1991) (Fig. 1). However, these epithelial sheets, without supporting substructures, are fragile, difficult to handle, and apt to contract (Clugston et al., 1991; Cooper et al., 1993). Advances in tissue engineering provide an alternative approach, since it permits the three-dimensional reconstruction of skin and oral mucosa, by culture of keratinocytes alone or with fibroblasts on dermal matrices in vitro (Fig. 2). Satisfactory clinical results have been reported for intra-oral transplantation of full-thickness engineered oral mucosa (Lauer and Schimming, 2001; Izumi et al., 2003a). It has also been shown that the use of a mucosal composite can assist in epithelial graft adherence and maturation, and minimize wound contraction and scarring (Cooper et al., 1993). Apart from clinical use, tissueengineered oral mucosa can be used as an in vitro test model for wound healing, mucotoxicity, and biocompatibility studies. Since tissueengineered in vitro models take the in vivo anatomical structure into account, they simulate the clinical situation better than do monolayer cell culture models (Schmalz, 2002). In the last decade, research has concentrated on the development and characterization of human oral mucosal equivalents by introducing new dermal scaffolds and epithelial cell culture methods. In this article, we review the strategies used for the production of three-dimensional human oral mucosal models and their applications. (II) NORMAL ORAL MUCOSA Received November 29, 2005; Accepted April 27, 2006 Oral mucosa consists of two distinct layers. The surface epithelium is supported by a fibrous connective tissue layer, the lamina propria. In many regions of the mouth, the oral mucosa is attached to underlying structures by a loose connective tissue component, the submucosa. These three layers are analogous to the epidermal, dermal, and hypodermal layers of the skin. The epithelial layer of the oral mucosa is stratified squamous epithelium, which may be keratinized or non-keratinized, according to the region of the mouth. The epithelium exhibits four layers of cells: the basal layer, spinous layer, granular layer, and the superficial layer, known as the cornified layer in the skin and the keratinized layer in oral mucosa. Keratinization involves the transformation of viable keratinocytes in the granular layer into dead surface cells devoid of organelles and packed with dense masses of cytokeratin filaments. In non-keratinized oral epithelium, the granular layer is replaced by the surface layer, the cells of which lack keratohyaline granules. Basal layer keratinocytes are progenitor cells that undergo terminal differentiation as they migrate to the surface. In addition to Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research 115 Moharamzadeh et al. 116 J Dent Res 86(2) 2007 Figure 1. Monolayer culture of human oral keratinocytes on a collagencoated flask. keratinocytes, oral epithelium contains non-keratinocyte clear cells: melanocytes, Langerhans cells, and Merkel cells. Adhesion between epithelial cells is achieved by desmosomes. The basal layers are attached to the underlying lamina propria through hemidesmosomes and the basement membrane, which contains collagen type IV, laminin, and fibronectin. Cytokeratins are intermediate filaments found in all types of epithelia, and are the most fundamental markers of epithelial differentiation. Cytokeratin profile reflects both cell type and differentiation status in different types and different layers of epithelia (Table 1). The lamina propria consists of an abundant network of type I collagen fibers, and the deeper layers contain collagen type III fibers and elastic fibers in various amounts, depending upon the site. Many fibroblasts are present, but only very occasional macrophages, plasma cells, mast cells, and lymphocytes are found. The lamina propria also contains vascular components, which form extensive capillary loops in the papillae between the epithelial ridges. Lymphatic vessels, nerves, and nerve endings are also present, as well as the ducts of salivary glands, whose acini are usually found in the deeper submucosa. Varying numbers of sebaceous glands are found in the oral cavity, but are not associated with hair follicles (Atkinson et al., 2000). Figure 2. Histological sections of (A) normal oral mucosa biopsy, (B) tissue-engineered skin, and (C) tissue-engineered oral mucosa. (III) CULTURED EPITHELIAL SHEETS (A) Monolayer human keratinocytes in serial culture in vitro, using a feeder layer composed of irradiated 3T3 mouse fibroblasts and a In 1975, Rheinwald and Green introduced a method to grow Table 1. Cytokeratin Expression in Different Layers of Oral Epithelium Cytokeratin Number Stratified squamous epithelial cell types Neutral-Basic (B, II): Acidic (A, I): 1 10 4 5 Keratinizing suprabasal cells Non-keratinizing intermediate and superficial cells Basal cells +++ - - + - +++ - +++ - 13 7 14 17 19 ++ - - + ++ +++ +++ - (++)* + * Basal cells in mucosa but not in skin. Patterns of cytokeratin expression: - no expression, + weak expression, ++ moderate expression, +++ strongly expressed. Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research 20 8 18 - - - - - - J Dent Res 86(2) 2007 Tissue-engineered Oral Mucosa specific culture medium called Green's medium. This method is frequently used for the culture of keratinocytes and production of single-layer epithelial sheets. Several investigators have been successful in culturing sheets of oral keratinocytes without an irradiated feeder layer (Arenholt-Bindslev et al., 1987; Lauer, 1994). As has been mentioned, these epithelial sheets are fragile, difficult to handle, and apt to contract. Monolayer cultures have been extremely helpful to our study of the basic biology, and responses to stimuli, of both oral and skin keratinocytes, and many studies have used them. However, the oral epithelium and epidermis are complex multilayer structures, with cells undergoing terminal differentiation, and monolayer cultures may not be a good model of what is happening in vivo. Thus, the development of a threedimensional multilayer culture system was a major breakthrough in epithelial biology and tissue engineering. (B) Multilayer The culture of keratinocytes on permeable cell culture membranes at the air/liquid interface facilitated the construction of multilayer sheets of epithelium, which resemble native epithelium and show signs of differentiation, such as basement membrane formation, different cytokeratin expression, and keratinization if the origin of the keratinocytes is keratinized mucosa (Rosdy and Clauss, 1990; Rosdy et al., 1993). A commercially available in vitro model of oral epithelium, developed by SkinEthic Laboratories (Nice, France), consists of a three-dimensional, multilayer culture of the human TR146 keratinocyte cell line on polycarbonate cell culture inserts. Since the cells are derived from an oral squamous cell carcinoma cell line, this tissue model does not fully differentiate, but does form a non-keratinizing oral epithelium that has been extensively used for biocompatibility and other studies. SkinEthic's other product, gingival epithelium, which is produced by air-liquid interface culture of normal gingival keratinocytes, produces a keratinized stratified squamous epithelium similar to normal gingival epithelium. EpiOral TM and EpiGingival TM were developed by MatTek Corp. (Ashland, MA, USA). These are three-dimensional reconstructs of human oral (buccal) and gingival epithelium that form multilayer, stratified non-keratinized and keratinized oral epithelium, respectively, which exhibit in vivo-like morphological and growth characteristics. Both tissue reconstructs express cytokeratin K13 and weakly express cytokeratin K14. They also produce naturally occurring antimicrobial peptides, including human beta defensins. (IV) CONNECTIVE TISSUE Fibroblasts, the most common cells in the connective tissue, can be easily isolated and cultured in monolayers by conventional cell culture techniques. It has been shown that fibroblasts cultured on three-dimensional porous scaffolds produce significantly higher levels of extracellular matrix than do fibroblasts grown in monolayers (Berthod et al., 1993). Newly synthesized collagen in three-dimensional cultures of fibroblasts can be characterized by transmission electron microscopy. Fibroblasts play an important role in epithelial morphogenesis, keratinocyte adhesion, and the formation of the complex dermal-epithelial junction (Saintigny et al., 1993). The epithelial phenotype and keratin expression are 117 extrinsically influenced by the nature and origin of the underlying fibroblasts (Okazaki et al., 2003) and the mesenchymal substrate (Merne and Syrjanen, 2003). It has been shown that without fibroblasts in the matrix, the epithelium ceases to proliferate (Fusenig, 1994), while differentiation continues (Smola et al., 1998). The significance of fibroblasts has also been shown by an experiment in which degenerative vacuolization was seen in co-cultures grown in the absence of fibroblasts. The use of oral buccal and vaginal fibroblasts led to a non-keratinized epithelium, in contrast to cultures with skin fibroblasts, which showed slight parakeratinization (Atula et al., 1997). Thus, fibroblasts may influence the differentiation potential of the epithelium toward that found at the site of origin of the fibroblasts. (V) FULL-THICKNESS ORAL MUCOSA ENGINEERING An ideal full-thickness engineered oral mucosa that resembles normal oral mucosa consists of (Fig. 2): (1) a lamina propria, which are comprised of a threedimensional scaffold infiltrated by fibroblasts producing extracellular matrix. This structure can be mimicked by the seeding of oral fibroblasts into a porous biocompatible scaffold, and long-term culturing in a fibroblast differentiation medium (Berthod et al., 1993; Black et al., 2005). Possible difficulties of such artificial structures include: poor fibroblast infiltration, due to the lack of porosity, the shrinkage of the scaffold if large numbers of fibroblasts are seeded, and rapid biodegradation of the scaffold. (2) a continuous basement membrane separating the lamina propria and the epithelium. The basement membrane can be characterized by transmission electron microscopy showing lamina lucida, lamina densa, and anchoring fibers. Immunostaining for basement membrane antigens—such as collagen type IV, laminin, fibronectin, integrins, and bullous pemphigoid antigen—is also a useful characterization method (Black et al., 2005). (3) a stratified squamous epithelium on the basement membrane, including densely packed keratinocytes that undergo differentiation as they migrate to the surface. This may be mimicked by the growth in culture of oral keratinocytes at the air-liquid interface in a chemically defined medium, which contains keratinocyte growth factors such as epidermal growth factor (EGF) (Izumi et al., 1999; Moriyama et al., 2001; Ophof et al., 2002; Rouabhia and Deslauriers, 2002; Bhargava et al., 2004). Significant issues that need to be addressed in the growth of multilayered epithelial constructs on connective tissue substrates include keratinocyte invasion into the connective tissue layer and poor differentiation of the epithelium. To address these problems and optimize the construction of full-thickness oral mucosa, one must consider many factors. These include the choice of (A) scaffold, (B) the cell source, and (C) the culture medium. (A) Scaffolds An important element in oral mucosa and skin reconstruction is the scaffold that supports the cells. Choosing the right scaffold with ideal biocompatibility, porosity, biostability, and mechanical properties is a crucial step in tissue engineering. Scaffolds used in oral mucosa and skin reconstruction fall into several different categories: (1) naturally derived Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research Moharamzadeh et al. 118 J Dent Res 86(2) 2007 Figure 4. The co-culture system developed by Moriyama et al. for fabricating composite cultured oral mucosa. Culture was performed at the air-liquid interface. (A) Keratinocytes; (B) fibroblasts; (C) collagen sponge and collagen gel; (D) millipore filter; and (E) steel mesh. being frozen; lyophilization; and ability to be preserved in glycerol (Heck et al., 1985; Krejci et al., 1991; McKay et al., 1994; Ghosh et al., 1997). It has been shown that oral mucosal substitutes composed of oral keratinocytes cultured on skinderived substrates (DED or AlloDerm) show histological and immunohistochemical characteristics very close to those of normal oral mucosa (Ophof et al., 2002). However, close examination of oral mucosal equivalents based on DED reveals very limited in vitro fibroblast infiltration in this scaffold, as compared with normal oral mucosa (Fig. 3B). Figure 3. De-epidermalized dermis (DED). (A) Macroscopic view. (B) Histological section of oral mucosa reconstructed on DED. scaffolds, such as acellular dermis and amniotic membrane; (2) fibroblast-populated skin substitutes; (3) collagen-based scaffolds; (4) gelatin-based scaffolds; (5) fibrin-based materials; (6) synthetic scaffolds, such as polymers; and (7) hybrid scaffolds, which are combinations of natural and synthetic matrices. Naturally Derived Scaffolds Acellular Dermis Acellular cadaveric dermis (AlloDermTM) was used by Izumi et al. (1999) as a scaffold for the tissue engineering of oral mucosa. AlloDerm is an acellular, non-immunogenic cadaveric human dermis (Rennekampff et al., 1997) that has a polarity by which one side has a basal lamina suitable for epithelial cells, and the other side has intact vessel channels suitable for fibroblast infiltration (Livesey et al., 1995). De-epidermalized dermis (DED) has been extensively utilized for the preparation of human epidermal-dermal composites (Ghosh et al., 1997; Chakrabarty et al., 1999; Ralston et al., 1999; Lee et al., 2000; Herson et al., 2001), and also for in vitro reconstruction of human hard palate mucosal epithelium (Cho et al., 2000) (Fig. 3). De-epithelialized bovine tongue mucosa has also been used as a substrate for keratinocyte culture in vitro (Hildebrand et al., 2002). DED is prepared from split-thickness skin by the removal of the epidermis and dermal fibroblasts from the dermis. The advantages that have made the DED a popular scaffold are: good durability and reduced antigenicity; ability to retain its structural properties, even after Amniotic Membrane The possibility of using human amniotic membrane as a substrate for culturing oral epithelial cells and its suitability for ocular surface reconstruction in rabbit has been examined previously (Nakamura et al., 2003). These investigators developed and characterized an engineered oral epithelium with numerous desmosomes and attached to a basement membrane with hemidesmosomes; the cells were able to express keratins 3, 4, and 13. Fibroblast-populated Skin Substitutes Fibroblast-populated scaffolds include several commercially available living skin equivalents. DermagraftTM, developed by Advanced Tissue Sciences Inc. (Coronado, CA, USA), is a dermal substitute composed of a biodegradable polymer mesh populated with dermal fibroblasts (Purdue, 1997). Another product, ApligrafTM (Graft skin), developed by Organogenesis, Inc. (Canton, MA, USA), is a composite graft composed of allogenic keratinocytes grown on a fibroblast-populated bovine collagen gel (Eaglstein et al., 1995; Gentzkow et al., 1996). Other living skin substitutes include Orcel TM (Ortec International Inc., New York, NY, USA), PolyactiveTM (HC Implants, Leiden, The Netherlands), and Hyalograf 3D TM (Fidia Advanced Biopolymers, Padua, Italy). The fibroblasts within these scaffolds proliferate and produce extracellular matrix and growth factors within 2-3 weeks, creating a dermislike matrix (Gentzkow et al., 1996). Collagen-based Scaffolds Pure Collagen Scaffolds In 1996, Masuda and colleagues developed the first in vitro full-thickness oral mucosal model by seeding cultured normal gingival keratinocytes on contracted bovine skin collagen gels Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research J Dent Res 86(2) 2007 Tissue-engineered Oral Mucosa (CCG) containing fibroblasts, and co-culturing in a reconstruction medium at an air-liquid interface for 10 days. They obtained a well-differentiated mucosal model, which was histologically similar to native tissues. Moriyama et al. (2001) modified this method and developed a composite cultured oral mucosa utilizing an atelopeptide type I collagen sponge matrix with CCG. Their mucosal model was composed of (1) a lamina propria in which fibroblasts were embedded in CCG and a honeycomb structured collagen sponge, and (2) stratified epithelial cell layers on the surface of the cultured lamina propria (Fig. 4). The benefit of this model is that the collagen gel supports fibroblasts, which provides a suitable substrate for keratinocyte multilayer formation, and prevents epithelial cell invasion and island formation in the connective tissue layer (MacCallum and Lillie, 1990). Laminin expression was detected between the epithelium and lamina propria in Moriyama's model. However, type IV collagen expression and hemidesmosome-like structure were not recognizable. Furthermore, the fibroblasts embedded in the collagen gel synthesized little extracellular matrix (ECM), compared with that synthesized on three-dimensional porous scaffolds (Berthod et al., 1993). Rouabhia and Deslauriers (2002) produced and characterized an in vitro engineered human oral mucosa using bovine skin collagen. Their method consisted of mixing bovine skin collagen with normal human oral fibroblasts to produce engineered lamina propria, and then seeding oral epithelial cells on this matrix and growing them at an air-liquid interface. In their mucosal model, epithelial cells expressed the proliferation marker Ki-67 as well as cytokeratins K14, K19, and the differentiation marker cytokeratin K10. Keratinocytes interacted with fibroblasts by secreting basement membrane proteins (laminins), and by expressing integrins (1 and ␣21). They also showed that the engineered oral mucosa was able to secrete interleukins (IL-1 and IL-8), tumor necrosis factor alpha (TNF-␣), and different metalloproteinases, such as gelatinase-A and gelatinase-B. As a scaffold, collagen matrix is very biocompatible, but it biodegrades rapidly and has poor mechanical properties. Crosslinking of the collagen-based scaffolds is an effective method to improve biostability and mechanical properties (Ma et al., 2003). However, cross-linking of collagen-based tissues enhances the tendency toward calcification, which is not desirable in clinical situations (Nimni, 1995). Compound Collagen Scaffolds Several compound collagen-based matrices have been introduced to improve the function of the scaffolds for tissue engineering. These include: the collagen-chitosan scaffold (Ma et al., 2003), collagen-elastin membrane (Hafemann et al., 1999), collagen-glucosaminoglycan (C-GAG) matrix (Ojeh et al., 2001), and collagen-GAG-chitosan (CGC) scaffolds (Vaissiere et al., 2000; Black et al., 2005). Chitosan is a naturally occurring substance that is chemically similar to cellulose and is derived from chitin, a polysaccharide found in the exoskeleton of shellfish-like shrimp or crabs. Chitosan functions as a bridge to increase the cross-linking efficiency of glutaraldehyde due to the longer chain of amino groups. Glycosaminoglycans are essential components of the extracellular matrix, composed of long, non-branched polymers of repeating disaccharide units, one of which is an amino sugar. Possible sources of GAGs include shark cartilage, bovine 119 trachea, and porcine cartilage. GAGs such as chondroitin sulfate and hyaluronic acid are hydrophilic, attracting large amounts of water and forming hydrated gels, enabling watersoluble molecules to diffuse rapidly (Atkinson et al., 2000). Fibroblasts grown within a CGC sponge express a significantly increased collagen synthesis, compared with that of fibroblasts embedded in a collagen gel and monolayer culture of fibroblasts (Berthod et al., 1993). Gelatin-based Scaffolds Gelatin-based materials such as gelatin-glucan (Lee et al., 2003), gelatin-hyaluronate (Choi et al., 1999a), and gelatinchitosan-hyaluronic acid (Mao et al., 2003) matrices have been developed for skin tissue engineering. The denatured form of collagen, gelatin, is non-antigenic, fibroblast-attractant, and a macrophage activator, and promotes epithelialization and granulation tissue formation (Choi et al., 1999a,b, 2001; Hong et al., 2001). Glucan is antibacterial, antiviral, and anticoagulant, and promotes wound-healing activity (Douwes, 2005). Hyaluronic acid is added to improve the biological and mechanical properties of these scaffolds (Mao et al., 2003). Fibrin-based Scaffolds Fibrin matrix has been used for the in vitro construction of human cartilage, skin, and bone (Ruszymah, 2004). BioseedTM, developed by BioTissue Technologies GmbH (Freiburg, Germany), is a skin substitute, composed of fibrin sealant with cultured autologous human keratinocytes. Fibrin glue matrix gives sufficient adherent stability to the grafted keratinocytes in an actively proliferating state. Further advantages are ease of reproducibility and grafting, as well as a reduction in operating time and costs (Kaiser et al., 1994). As mentioned above, natural materials possess many advantages that have made them popular as scaffolds for tissue engineering. However, these materials also have some disadvantages. Many of them are isolated from human or animal tissue, and are not available in large quantities. They suffer from large batch-to-batch variations, and are typically expensive. Additionally, these materials exhibit a limited range of physical properties. These drawbacks have led some researchers to consider using synthetic materials to fabricate matrices for use in tissue engineering of skin and oral mucosa. Synthetic Scaffolds Polycarbonate-permeable membranes are used in commercially available partial-thickness epithelial models (SkinEthic and MatTek tissue models). Successful use of a biodegradable segmented co-polymer of poly (ethyleneglycolterephthalate)poly (butylene terephthalate) (PEGT/PBT) in skin tissue engineering has been reported (El-Ghalbzouri et al., 2004). This synthetic scaffold has good mechanical properties, and there is no risk of disease transmission. However, incorporation of fibroblast-populated collagen or fibrin into the pores of the scaffold is required for better results. Porous polylactic glycolic acid scaffold has also been used to construct a lining mucosa in a tissue-engineered prosthetic mucosa for replacement of a tracheal defect (Kim et al., 2004). A dermal scaffold composed of knitted poly (lactic-co-glycolic acid) (10:90)-poly (caprolactone) (PLGA-PCL) mesh has shown superior results in terms of cell distribution and tissue formation, compared with results from three natural scaffolds, including equine collagen foam, AlloDerm, and Chitosan (Ng et al., 2004). Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research Moharamzadeh et al. 120 J Dent Res 86(2) 2007 Table 2. Tissue-engineered Oral Mucosa Equivalents Reference Cell/Medium Scaffold Application Masuda, 1996 Normal gingival fibroblasts and keratinocytes/DMEM plus FCS and CaCl2 added KGM* Contracted collagen gel Development Schmalz et al., 1997 Oral keratinocyte and fibroblast co-culture/DMEM plus FCS Nylon mesh Biocompatibility testing Izumi et al., 1999 Oral fibroblasts and keratinocytes/FCS containing MCDB-153 medium AlloDerm Development Izumi et al., 2000 Oral fibroblasts and keratinocytes/serum-free culture medium AlloDerm Development Schmalz et al., 2000 TR146 cells from buccal SCC/DMEM plus FCS Polycarbonate filters Biocompatibility testing Cho et al., 2000 Palatal epithelial cells/DMEM and Ham's F12 medium plus FCS DED Development Moriyama et al., 2001 Gingival fibroblasts and keratinocytes/serum containing KGM Contracted collagen gel and collagen sponge matrix Development Navarro et al., 2001 Oral mucosal keratinocytes/DMEM and Ham's F12 medium plus FCS Cross-linked collagen-GAG matrices Optimization Rouabhia and Deslauriers, 2002 Oral epithelial cells/DMEM and Ham's F12 medium plus FCS Bovine skin collagen Development Mostefaoui et al., 2002 Oral epithelial cells/DMEM and Ham's F12 medium plus FCS Collgen matrix Biocompatibility testing Ophof et al., 2002 Oral keratinocytes/DMEM and Ham's F12 medium plus FCS Alloderm, DED, collagen type-I, collagen-elastin, and collagen-GAG Development and comparison Hildebrand et al., 2002 Normal epithelial keratinocytes/serum-containing culture medium De-epithelialized bovine tongue mucosa Development and characterization Nakamura et al., 2003 Rabbit oral mucosal cells/serum-containing culture medium Human amniotic membrane Clinical (ocular reconstruction) Izumi et al., 2003a,b Oral fibroblasts and keratinocytes/serum-free culture medium AlloDerm Clinical (intra-oral grafting) Bhargava et al., 2004 Buccal keratinocytes and fibroblasts/Green's medium DED Clinical (substitution urethroplasty) Andrian et al., 2004 Oral epithelial cells/DMEM and Ham's F12 medium plus FCS Bovine skin collagen In vitro (tissue invasion study) Claveau et al., 2004 Mostefaoui et al., 2004a,b Tardif et al., 2004 Oral epithelial cells/DMEM and Ham's F12 medium plus FCS Collgen matrix In vitro (Candida studies) Iida et al., 2005 Oral mucosal cells/chemically defined medium Acellular allogenic dermal matrix Clinical (burn treatment) * KGM = keratinocyte growth medium, SCC = squamous cell carcinoma. DMEM = Dulbecco’s modified Eagle medium. FCS = Fetal calf serum. SCC = Squamous cell carcinoma. DED = De-epidermalized dermis. GAG = Glycosaminoglycans. Hybrid Scaffolds A skin substitute based on a semi-synthetic scaffold made of benzyl ester of hyaluronan (HYAFF and Laserskin) has been developed. This scaffold has good in vitro and in vivo biocompatibility and controlled biodegradability (Zacchi et al., 1998). A hybrid scaffold of poly (lactic-co-glycolic acid)collagen has recently been used for dermal tissue engineering, but it has shown greater contraction compared with collagenhyaluronic acid foam (Ng et al., 2005). In a recent study comparing three different types of dermal scaffolds, a more efficient connective tissue formation was observed with use of a compression-molded/salt-leached PEGT/PBT copolymer, in comparison with lyophilized crosslinked collagen, and collagen-PEGT/PBT hybrid scaffolds. It was also shown that the thickness, porosity, and interconnecting pore size are important parameters in the ability of synthetic scaffolds to control connective tissue formation (Wang et al., 2005). fibroblasts and keratinocytes. Fibroblasts are usually isolated from the dermal layer of the skin or by oral mucosal biopsy, and are used at early passages for tissue engineering, because the extracellular matrix production by dermal fibroblasts decreases as the passage number increases (Takeda et al., 1992; Khorramizadeh et al., 1999). Keratinocytes can be obtained from different sites of the oral cavity, such as the hard palate (Cho et al., 2000), gingiva (Yoshizawa et al., 2004), or buccal mucosa (Bhargava et al., 2004). Normal human keratinocytes should also be used at very early passages, but immortalized human keratinocytes, such as HaCaT cells (Boelsma et al., 1999) or TR146 cells (Schmalz et al., 2000), can be used at extended passages in the reconstruction of oral mucosal test models. However, epidermal differentiation of transformed keratinocytes is not perfect, since the ultimate steps of terminal differentiation do not occur (Boelsma et al., 1999), and tumorderived cells are abnormal and not suitable for clinical use. (B) Cell Source Another important factor that must be considered in oral mucosa and skin reconstruction is the type and origin of (C) Culture Medium The commonly used culture medium for oral mucosa reconstruction is Dulbecco's modified Eagle medium (DMEM)Ham's F-12 medium (3:1), supplemented with fetal calf serum Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research J Dent Res 86(2) 2007 Tissue-engineered Oral Mucosa (FCS), glutamine, epidermal growth factor (EGF), hydrocortisone, adenine, insulin, transferrin, tri-iodothyronine, fungizone, penicillin, and streptomycin. In 2000, Izumi et al. developed and characterized a tissueengineered human oral mucosal equivalent using a serum-free culture method. In that study, they eliminated the use of serum and irradiated mouse fibroblast feeder layers, to minimize the exposure of human graft recipients to xenogenetic DNA or slow viruses that might be present in irradiated mouse 3T3 cells and serum, respectively. Yoshizawa et al. (2004) used the same technique to produce human conjunctiva and oral mucosa equivalents. It has been demonstrated that perfusion of oral keratinocytes with medium further enhanced cell viability and proliferation when cultured in a porous three-dimensional matrix of collagen-GAG cross-linked with glutaraldehyde (Navarro et al., 2001). A summary of different tissue-engineered oral mucosal models, their cells, culture systems, scaffolds, and their applications is shown in Table 2. (VI) APPLICATIONS OF ENGINEERED ORAL MUCOSA There are generally two major applications for tissueengineered oral mucosa: (1) clinical applications, and (2) as in vitro test systems and models. It is important to realize that tissue-engineering approaches may be different for each purpose. As an example, for clinical applications such as grafting, transplantation, and guided tissue regeneration, a biodegradable scaffold with optimal mechanical properties is desirable, because it will be replaced by the host tissue, and it must resist natural forces in the oral cavity, while a nonbiodegradable scaffold may result in a foreign body reaction. Also, transmission of infection and tissue rejection are major issues. Tumor-derived or virally transformed cell lines are precluded from clinical use, and high standards of tissue production and quality control are essential. However, these are less of a problem for an in vitro test model. Indeed, the need for reproducibility and lack of batch-to-batch variability may make the use of tumor and virally transformed cell lines desirable in this case. The scaffold should have maximum biostability to maintain its structure throughout the testing procedure. Depending on the biological endpoint, both epithelium-only and full-thickness oral mucosal models may have a use for in vitro tests. (A) Clinical Applications Skin Substitutes Currently, there is a variety of different commercially available skin substitutes for clinical applications. For example, DermagraftTM is used for temporary wound coverage of burns, and is then removed and replaced with autologous skin grafts (Purdue, 1997). Another product, Apligraf TM , has been successful in the treatment of venous ulcers (Gentzkow et al., 1996) and acute wounds (Eaglstein et al., 1995). It has been reported that tissue-engineered skin can affect the host cells and promotes tissue regeneration and remodeling by producing several cytokines and growth factors, such as IL-1, IL-3, IL-6, IL-8, transforming growth factors ␣ and , and fibroblast growth factor (Lee, 2000). Compared with engineered skin, tissue-engineered human oral mucosa has not yet been commercialized for clinical 121 applications. However, clinical studies have been carried out with tissue-engineered oral mucosal equivalents for intra- and extra-oral treatment, with favorable histological and clinical results. Intra-oral Applications Full-thickness engineered human oral mucosa can be used in periodontal peri-implant reconstruction and maxillofacial reconstructive surgery. Izumi et al. (2003a) reported a 100% "take" rate with intra-oral grafting of engineered oral mucosa. In their study, the engineered grafts showed clinical changes indicating vascular ingrowth, and had cytologic evidence of the persistence of grafted cultured keratinocytes on the surface. The graft enhanced the maturation of the underlying submucosal layer associated with rapid epithelial coverage. In vitro labeling of cultured and subsequently grafted gingival keratinocytes showed that the transplanted keratinocytes integrated into the newly formed mucosal epithelium (Lauer and Schimming, 2001). It has also been reported that the presence of an intact and viable epithelium influences secondary in vivo remodeling within the connective tissue layer of transplanted engineered oral mucosa, by synthesis and release of cytokines, enzymes, and growth factors (Izumi et al., 2003b). Extra-oral Applications In recent years, several tissue-engineered oral mucosa equivalents have been developed for extra-oral applications. Bhargava et al. (2004) reported the successful culture of a fullthickness tissue-engineered buccal mucosa, based on DED, with good mechanical properties for substitution urethroplasty. Autologous transplantation of cultivated oral epithelium on human amniotic membrane has been suggested as a feasible method for ocular surface reconstruction (Nakamura et al., 2003). Yoshizawa et al. (2004) developed and characterized human conjunctiva and oral mucosa equivalents, and suggested their use as graft materials for eyelid reconstruction. Lately, the application of a tissue-engineered human oral mucosal equivalent, based on an acellular allogenic dermis, for the treatment of a burn wound with satisfactory outcome has been reported (Iida et al., 2005). Compared with the transplantation of autologous keratinocytes alone, full-thickness engineered mucosa grafting results in better and faster wound healing of oral tissues. Longterm clinical follow-up of transplanted engineered oral mucosa has established this technique as an excellent additional tool in oral and maxillofacial surgery (Lauer and Schimming, 2002). However, the commercialization of engineered oral mucosa for clinical applications is restricted, due to the limitations in manufacturing facilities, governmental regulatory issues, and low profitability. Since the best cells for the patients are their own cells, the use of allogenic cells is not desirable, especially when most of the indications for many engineered oral mucosal grafts are not as urgent as the use of skin substitutes in lifethreatening situations, such as extensive burns. Therefore, tissue-engineered oral mucosa for clinical applications can be marketed only as a service with limited profitability. (B) In vitro Applications In vitro applications of three-dimensional oral mucosal models include biocompatibility testing and oral biology research studies, such as disease modeling and wound healing. Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research 122 Moharamzadeh et al. Figure 5. Different biological endpoints for the in vitro assessment of the response of engineered oral mucosa to an applied stimulus. Figure 7. Lymphocytes incorporated into tissue-engineered oral epithelium. Biocompatibility Testing Several studies have indicated the use of engineered oral mucosal models based on collagen membranes and synthetic polymers as in vitro test models, to evaluate the biological effects of biomaterials. Mostefaoui et al. (2002), using a reconstructed human oral mucosal model on a bovine collagen membrane, examined the effects of dentifrices on tissue structure and pro-inflammatory mediator released by epithelial cells. Schmalz et al. studied mucosal irritancy of metals used in dentistry by introducing these materials onto three-dimensional fibroblast-keratinocyte co-cultures on nylon mesh (1997), and also by a 3-D culture of TR146 cells grown on polycarbonate filters (2000). A similar epithelial model has been used by several investigators to evaluate the effects of mercury chloride (Khawaja et al., 2002) and different surfactants (Lundqvist et al., 2002; Hagi-Pavli et al., 2004) on epithelial viability and cytokine release from the epithelium. These in vitro models seem promising for mucotoxicity evaluation of dental biomaterials, since they reflect the clinical situation better than do single-layer cell culture test models. Therefore, they can reduce the need for animal testing and be more specific. Furthermore, such models allow investigators to study multiple responses of the epithelium or mucosa to different stimuli (Fig. 5). This is particularly valuable in the testing of responses to different biomaterials, oral healthcare products, etc., as well as in studies investigating the response of the oral epithelium or mucosa to bacteria and other disease processes. Tissue-engineered Models of Oral Disease The availability of well-characterized engineered tissue models J Dent Res 86(2) 2007 Figure 6. Histological picture of Candida albicans colonization and invasion of tissue-engineered oral epithelium. has led to the development of a new approach to the study of disease processes, and the development of tissue-engineered models of disease. With respect to the oral mucosa, tissueengineered oral mucosal models have been used to assess tissue invasion by Porphyromonas gingivalis (Andrian et al., 2004) in a model of gingivitis, and to evaluate the response of the oral mucosa to Candida albicans infection, such as changes in basement membrane proteins, matrix metalloproteinase deregulation (Claveau et al., 2004), and inflammatory marker release (Mostefaoui et al., 2004a,b; Tardif et al., 2004; Thornhill et al., 2005) (Fig. 6). Further research is in progress with regard to models of oral mucosal HIV infection and transmission (Nittayananta et al., 2004), and other disease models are currently under development. (VII) FUTURE DEVELOPMENTS Research on the optimization of oral mucosal equivalents is still in progress, and scientists are trying to simulate native oral mucosa as closely as possible, by developing new types of natural scaffolds, including most of the extracellular matrix elements, or synthetic scaffolds with optimized porosity and biodegradability. Other developments to reflect the in vivo situation more accurately include the incorporation of other types of cells, including endothelial cells, to promote angiogenesis and revascularization (Sahota et al., 2004), and immune cells such as lymphocytes (Fig. 7), monocytes, and Langerhans cells, to reproduce and evaluate immune responses. The development of tissue-engineered models of oral disease will also enhance our understanding of disease processes and the discovery of new treatments. REFERENCES Andrian E, Grenier D, Rouabhia M (2004). In vitro models of tissue penetration and destruction by Porphyromonas gingivalis. Infect Immun 72:4689-4698. Arenholt-Bindslev D, Jepsen A, MacCallum DK, Lillie JH (1987). The growth and structure of human oral keratinocytes in culture. J Invest Dermatol 88:314-319. Atkinson ME, Jowett A, White FH (2000). Principles of anatomy and oral anatomy for dental students. Taddington: Cava Cadavers. Atula S, Grenman R, Syrjanen S (1997). Fibroblasts can modulate the phenotype of malignant epithelial cells in vitro. Exp Cell Res 235:180- Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research J Dent Res 86(2) 2007 Tissue-engineered Oral Mucosa 187. Berthod F, Hayek D, Damour O, Collombel C (1993). Collagen synthesis by fibroblasts cultured within a collagen sponge. Biomaterials 14:749-754. Bhargava S, Chapple CR, Bullock AJ, Layton C, MacNeil S (2004). Tissueengineered buccal mucosa for substitution urethroplasty. BJU Int 93:807-811. Black AF, Bouez C, Perrier E, Schlotmann K, Chapuis F, Damour O (2005). Optimization and characterization of an engineered human skin equivalent. Tissue Eng 11:723-733. Boelsma E, Verhoeven MC, Ponec M (1999). Reconstruction of a human skin equivalent using a spontaneously transformed keratinocyte cell line (HaCaT). J Invest Dermatol 112:489-498. Chakrabarty KH, Dawson RA, Harris P, Layton C, Babu M, Gould L, et al. (1999). Development of autologous human dermal-epidermal composites based on sterilized human allodermis for clinical use. Br J Dermatol 141:811-823. Cho KH, Ahn HT, Park KC, Chung JH, Kim SW, Sung MW, et al. (2000). Reconstruction of human hard-palate mucosal epithelium on deepidermized dermis. J Dermatol Sci 22:117-124. Choi YS, Hong SR, Lee YM, Song KW, Park MH, Nam YS (1999a). Study on gelatin-containing artificial skin: I. Preparation and characteristics of novel gelatin-alginate sponge. Biomaterials 20:409-417. Choi YS, Hong SR, Lee YM, Song KW, Park MH, Nam YS (1999b). Studies on gelatin-containing artificial skin: II. Preparation and characterization of cross-linked gelatin-hyaluronate sponge. J Biomed Mater Res 48:631-639. Choi YS, Lee SB, Hong SR, Lee YM, Song KW, Park MH (2001). Studies on gelatin-based sponges. Part III: a comparative study of cross-linked gelatin/alginate, gelatin/hyaluronate and chitosan/hyaluronate sponges and their application as a wound dressing in full-thickness skin defect of rat. J Mater Sci Mater Med 12:67-73. Claveau I, Mostefaoui Y, Rouabhia M (2004). Basement membrane protein and matrix metalloproteinase deregulation in engineered human oral mucosa following infection with Candida albicans. Matrix Biol 23:477-486. Clugston PA, Snelling CF, Macdonald IB, Maledy HL, Boyle JC, Germann E, et al. (1991). Cultured epithelial autografts: three years of clinical experience with eighteen patients. J Burn Care Rehabil 12:533-539. Cooper ML, Andree C, Hansbrough JF, Zapata-Sirvent RL, Spielvogel RL (1993). Direct comparison of a cultured composite skin substitute containing human keratinocytes and fibroblasts to an epidermal sheet graft containing human keratinocytes on athymic mice. J Invest Dermatol 101:811-819. Douwes J (2005). (1-->3)-Beta-D-glucans and respiratory health: a review of the scientific evidence. Indoor Air 15:160-169. Eaglstein WH, Iriondo M, Laszlo K (1995). A composite skin substitute (graftskin) for surgical wounds. A clinical experience. Dermatol Surg 21:839-843. El-Ghalbzouri A, Lamme EN, van Blitterswijk C, Koopman J, Ponec M (2004). The use of PEGT/PBT as a dermal scaffold for skin tissue engineering. Biomaterials 25:2987-2996. Fusenig NE (1994). Epithelial-mesenchymal interactions regulate keratinocyte growth and differentiation in vitro. In: The keratinocyte handbook. Leigh IM, Lane EB, Watt FM, editors. Cambridge: University Press, pp. 71-94. Gentzkow GD, Iwasaki SD, Hershon KS, Mengel M, Prendergast JJ, Ricotta JJ, et al. (1996). Use of dermagraft, a cultured human dermis, to treat diabetic foot ulcers. Diabetes Care 19:350-354. Ghosh MM, Boyce S, Layton C, Freedlander E, Mac Neil S (1997). A comparison of methodologies for the preparation of human epidermaldermal composites. Ann Plast Surg 39:390-404. Hafemann B, Ensslen S, Erdmann C, Niedballa R, Zuhlke A, Ghofrani K, et al. (1999). Use of a collagen/elastin-membrane for the tissue engineering of dermis. Burns 25:373-384. Hagi-Pavli E, Williams D, Thornhill MH, Adams G, Smith S, Cruchley A (2004). The effect of different surfactants on epithelial haemostasis (abstract). J Dent Res 83(Spec Iss A):1230 (http://iadr.confex.com/iadr/ 2004Hawaii/techprogram/abstract_47103.htm). Heck EL, Bergstresser PR, Baxter CR (1985). Composite skin graft: frozen dermal allografts support the engraftment and expansion of autologous epidermis. J Trauma 25:106-112. 123 Herson MR, Mathor MB, Altran S, Capelozzi VL, Ferreira MC (2001). In vitro construction of a potential skin substitute through direct human keratinocyte plating onto decellularized glycerol-preserved allodermis. Artif Organs 25:901-906. Hildebrand HC, Hakkinen L, Wiebe CB, Larjava HS (2002). Characterization of organotypic keratinocyte cultures on deepithelialized bovine tongue mucosa. Histol Histopathol 17:151-163. Hong SR, Lee SJ, Shim JW, Choi YS, Lee YM, Song KW, et al. (2001). Study on gelatin-containing artificial skin IV: a comparative study on the effect of antibiotic and EGF on cell proliferation during epidermal healing. Biomaterials 22:2777-2783. Iida T, Takami Y, Yamaguchi R, Shimazaki S, Harii K (2005). Development of a tissue-engineered human oral mucosa equivalent based on an acellular allogeneic dermal matrix: a preliminary report of clinical application to burn wounds. Scand J Plast Reconstr Surg Hand Surg 39:138-146. Izumi K, Takacs G, Terashi H, Feinberg SE (1999). Ex vivo development of a composite human oral mucosal equivalent. J Oral Maxillofac Surg 57:571-577; discussion 577-578. Izumi K, Terashi H, Marcelo CL, Feinberg SE (2000). Development and characterization of a tissue-engineered human oral mucosa equivalent produced in a serum-free culture system. J Dent Res 79:798-805. Izumi K, Feinberg SE, Iida A, Yoshizawa M (2003a). Intraoral grafting of an ex vivo produced oral mucosa equivalent: a preliminary report. Int J Oral Maxillofac Surg 32:188-197. Izumi K, Feinberg SE, Terashi H, Marcelo CL (2003b). Evaluation of transplanted tissue-engineered oral mucosa equivalents in severe combined immunodeficient mice. Tissue Eng 9:163-174. Kaiser HW, Stark GB, Kopp J, Balcerkiewicz A, Spilker G, Kreysel HW (1994). Cultured autologous keratinocytes in fibrin glue suspension, exclusively and combined with STS-allograft (preliminary clinical and histological report of a new technique). Burns 20:23-29. Khawaja NA, Lundqvist CK, Cruchley AT, Williams DM, Thornhill MH (2002). HgCl2 induces IL-6 and IL-8 production in a stratified oral mucosal culture system (abstract). J Dent Res 81(Spec Iss A):496. Khorramizadeh MR, Tredget EE, Telasky C, Shen Q, Ghahary A (1999). Aging differentially modulates the expression of collagen and collagenase in dermal fibroblasts. Mol Cell Biochem 194:99-108. Kim J, Suh SW, Shin JY, Kim JH, Choi YS, Kim H (2004). Replacement of a tracheal defect with a tissue-engineered prosthesis: early results from animal experiments. J Thorac Cardiovasc Surg 128:124-129. Krejci NC, Cuono CB, Langdon RC, McGuire J (1991). In vitro reconstitution of skin: fibroblasts facilitate keratinocyte growth and differentiation on acellular reticular dermis. J Invest Dermatol 97:843848. Lauer G (1994). Autografting of feeder-cell free cultured gingival epithelium. Method and clinical application. J Craniomaxillofac Surg 22:18-22. Lauer G, Schimming R (2001). Tissue-engineered mucosa graft for reconstruction of the intraoral lining after freeing of the tongue: a clinical and immunohistologic study. J Oral Maxillofac Surg 59:169175; discussion 175-177. Lauer G, Schimming R (2002). [Clinical application of tissue-engineered autologous oral mucosa transplants]. Mund Kiefer Gesichtschir 6:379393 [article in German]. Lauer G, Otten JE, von Specht BU, Schilli W (1991). Cultured gingival epithelium. A possible suitable material for pre-prosthetic surgery. J Craniomaxillofac Surg 19:21-26. Lee DY, Ahn HT, Cho KH (2000). A new skin equivalent model: dermal substrate that combines de-epidermized dermis with fibroblastpopulated collagen matrix. J Dermatol Sci 23:132-137. Lee KH (2000). Tissue-engineered human living skin substitutes: development and clinical application. Yonsei Med J 41:774-779. Lee SB, Jeon HW, Lee YW, Lee YM, Song KW, Park MH, et al. (2003). Bio-artificial skin composed of gelatin and (1-->3), (1-->6)-betaglucan. Biomaterials 24:2503-2511. Livesey SA, Herndon DN, Hollyoak MA, Atkinson YH, Nag A (1995). Transplanted acellular allograft dermal matrix. Potential as a template for the reconstruction of viable dermis. Transplantation 60:1-9. Lundqvist CK, Thornhill MH, Williams DM, Smith S, Cruchley AT (2002). The effect of sodium lauryl sulphate on epithelial homeostasis Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research 124 Moharamzadeh et al. (abstract). J Dent Res 81(Spec Iss A):3054. Ma L, Gao C, Mao Z, Zhou J, Shen J, Hu X, et al. (2003). Collagen/chitosan porous scaffolds with improved biostability for skin tissue engineering. Biomaterials 24:4833-4841. MacCallum DK, Lillie JH (1990). Evidence for autoregulation of cell division and cell transit in keratinocytes grown on collagen at an airliquid interface. Skin Pharmacol 3:86-96. Madden MR, Finkelstein JL, Staiano-Coico L, Goodwin CW, Shires GT, Nolan EE, et al. (1986). Grafting of cultured allogeneic epidermis on second- and third-degree burn wounds on 26 patients. J Trauma 26:955-962. Mao JS, Liu HF, Yin YJ, Yao KD (2003). The properties of chitosan-gelatin membranes and scaffolds modified with hyaluronic acid by different methods. Biomaterials 24:1621-1629. Masuda I (1996). [An in vitro oral mucosal model reconstructed from human normal gingival cells]. Kokubyo Gakkai Zasshi 63:334-353 [article in Japanese]. McKay I, Woodward B, Wood K, Navsaria HA, Hoekstra H, Green C (1994). Reconstruction of human skin from glycerol-preserved allodermis and cultured keratinocyte sheets. Burns 20(Suppl 1):S19S22. Merne M, Syrjanen S (2003). The mesenchymal substrate influences the epithelial phenotype in a three-dimensional cell culture. Arch Dermatol Res 295:190-198. Moriyama T, Asahina I, Ishii M, Oda M, Ishii Y, Enomoto S (2001). Development of composite cultured oral mucosa utilizing collagen sponge matrix and contracted collagen gel: a preliminary study for clinical applications. Tissue Eng 7:415-427. Mostefaoui Y, Claveau I, Ross G, Rouabhia M (2002). Tissue structure, and IL-1beta, IL-8, and TNF-alpha secretions after contact by engineered human oral mucosa with dentifrices. J Clin Periodontol 29:1035-1041. Mostefaoui Y, Bart C, Frenette M, Rouabhia M (2004a). Candida albicans and Streptococcus salivarius modulate IL-6, IL-8, and TNF-alpha expression and secretion by engineered human oral mucosa cells. Cell Microbiol 6:1085-1096. Mostefaoui Y, Claveau I, Rouabhia M (2004b). In vitro analyses of tissue structure and interleukin-1beta expression and production by human oral mucosa in response to Candida albicans infections. Cytokine 25:162-171. Nakamura T, Endo K, Cooper LJ, Fullwood NJ, Tanifuji N, Tsuzuki M, et al. (2003). The successful culture and autologous transplantation of rabbit oral mucosal epithelial cells on amniotic membrane. Invest Ophthalmol Vis Sci 44:106-116. Navarro FA, Mizuno S, Huertas JC, Glowacki J, Orgill DP (2001). Perfusion of medium improves growth of human oral neomucosal tissue constructs. Wound Repair Regen 9:507-512. Ng KW, Khor HL, Hutmacher DW (2004). In vitro characterization of natural and synthetic dermal matrices cultured with human dermal fibroblasts. Biomaterials 25:2807-2818. Ng KW, Tham W, Lim TC, Werner Hutmacher D (2005). Assimilating cell sheets and hybrid scaffolds for dermal tissue engineering. J Biomed Mater Res A 75:425-438. Nimni ME (1995). Collagen: molecular structure and biomaterial properties. In: Encyclopedic handbook of biomaterials and bioengineering. Part A: Materials. Wise DL, editor. New York: Marcel Dekker Inc., pp. 12291243. Nittayananta W, Coombs RW, Ayehunie S, Klausner M, Dale BA (2004). Development of a human oral epithelial tissue model to study HIV transmission and the role of beta-defensins. XV International AIDS Conference, Bangkok, Thailand, July 11-16. Ojeh NO, Frame JD, Navsaria HA (2001). In vitro characterization of an artificial dermal scaffold. Tissue Eng 7:457-472. Okazaki M, Yoshimura K, Suzuki Y, Harii K (2003). Effects of subepithelial fibroblasts on epithelial differentiation in human skin and oral mucosa: heterotypically recombined organotypic culture model. Plast Reconstr Surg 112:784-792. Ophof R, van Rheden RE, Von den Hoffa JW, Schalkwijk J, Kuijpers- Jagtman AM (2002). Oral keratinocytes cultured on dermal matrices form a mucosa-like tissue. Biomaterials 23:3741-3748. Purdue GF (1997). Dermagraft-TC pivotal efficacy and safety study. J Burn Care Rehabil 18:S13-S14. Ralston DR, Layton C, Dalley AJ, Boyce SG, Freedlander E, Mac Neil S (1999). The requirement for basement membrane antigens in the production of human epidermal/dermal composites in vitro. Br J Dermatol 140:605-615. Rennekampff HO, Kiessig V, Griffey S, Greenleaf G, Hansbrough JF (1997). Acellular human dermis promotes cultured keratinocyte engraftment. J Burn Care Rehabil 18:535-544. Rheinwald JG, Green H (1975). Serial cultivation of strains of human epidermal keratinocytes: the formation of keratinizing colonies from single cells. Cell 6:331-343. Rosdy M, Clauss LC (1990). Terminal epidermal differentiation of human keratinocytes grown in chemically defined medium on inert filter substrates at the air-liquid interface. J Invest Dermatol 95:409-414. Rosdy M, Pisani A, Ortonne JP (1993). Production of basement membrane components by a reconstructed epidermis cultured in the absence of serum and dermal factors. Br J Dermatol 129:227-234. Rouabhia M, Deslauriers N (2002). Production and characterization of an in vitro engineered human oral mucosa. Biochem Cell Biol 80:189-195. Ruszymah BH (2004). Autologous human fibrin as the biomaterial for tissue engineering. Med J Malaysia 59(Suppl B):30-31. Sahota PS, Burn JL, Brown NJ, MacNeil S (2004). Approaches to improve angiogenesis in tissue-engineered skin. Wound Repair Regen 12:635-642. Saintigny G, Bonnard M, Damour O, Collombel C (1993). Reconstruction of epidermis on a chitosan cross-linked collagen-GAG lattice: effect of fibroblasts. Acta Derm Venereol 73:175-180. Schmalz G (2002). Materials science: biological aspects. J Dent Res 81:660663. Schmalz G, Arenholt-Bindslev D, Hiller KA, Schweikl H (1997). Epithelium-fibroblast co-culture for assessing mucosal irritancy of metals used in dentistry. Eur J Oral Sci 105:86-91. Schmalz G, Schweikl H, Hiller KA (2000). Release of prostaglandin E2, IL6 and IL-8 from human oral epithelial culture models after exposure to compounds of dental materials. Eur J Oral Sci 108:442-448. Smola H, Stark HJ, Thiekotter G, Mirancea N, Krieg T, Fusenig NE (1998). Dynamics of basement membrane formation by keratinocyte-fibroblast interactions in organotypic skin culture. Exp Cell Res 239:399-410. Takeda K, Gosiewska A, Peterkofsky B (1992). Similar, but not identical, modulation of expression of extracellular matrix components during in vitro and in vivo aging of human skin fibroblasts. J Cell Physiol 153:450-459. Tardif F, Goulet JP, Zakrazewski A, Chauvin P, Rouabhia M (2004). Involvement of interleukin-18 in the inflammatory response against oropharyngeal candidiasis. Med Sci Monit 10:BR239-BR249. Thornhill MH, Cruchley A, Lopez-Ribot J, Allaker AP (2005). In vitro modeling of oral candidiasis (abstract). J Dent Res 84(Special Iss A):318 (http://iadr.confex.com/iadr/2005Balt/techprogram/ abstract_59260.htm). Ueda M, Ebata K, Kaneda T (1991). In vitro fabrication of bioartificial mucosa for reconstruction of oral mucosa: basic research and clinical application. Ann Plast Surg 27:540-549. Vaissiere G, Chevallay B, Herbage D, Damour O (2000). Comparative analysis of different collagen-based biomaterials as scaffolds for long-term culture of human fibroblasts. Med Biol Eng Comput 38:205-210. Wang H, Pieper J, Peters F, van Blitterswijk CA, Lamme EN (2005). Synthetic scaffold morphology controls human dermal connective tissue formation. J Biomed Mater Res A 74:523-532. Yoshizawa M, Feinberg SE, Marcelo CL, Elner VM (2004). Ex vivo produced human conjunctiva and oral mucosa equivalents grown in a serum-free culture system. J Oral Maxillofac Surg 62:980-988. Zacchi V, Soranzo C, Cortivo R, Radice M, Brun P, Abatangelo G (1998). In vitro engineering of human skin-like tissue. J Biomed Mater Res 40:187-194. Downloaded from jdr.sagepub.com at Sheffield University on March 9, 2011 For personal use only. No other uses without permission. International and American Associations for Dental Research View publication stats J Dent Res 86(2) 2007