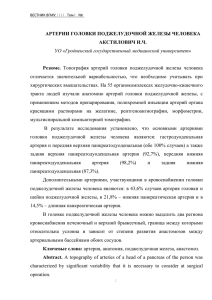
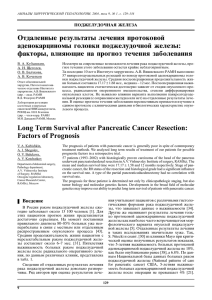
Surg Radiol Anat DOI 10.1007/s00276-014-1276-8 Original Article The superior horizontal pancreatic artery of Popova: a review and an anatomoradiological study of an important morphological variant of the pancreatica magna artery S. Mosca · F. Di Gregorio · M. Regoli · E. Bertelli Received: 10 December 2013 / Accepted: 17 February 2014 © Springer-Verlag France 2014 Abstract Purpose The superior horizontal pancreatic artery was described in 1910, and after a few years, it was forgot by most investigators. This research is aimed to revive the description of this artery, describing course, pattern of branching and frequency. Methods More than 1,000 of angiographies including studies of the superior mesenteric artery, celiac trunk and its branches, were selected from the angiographic archives of the ex-institutes of Radiology of Siena, Rome (University of Sacro Cuore) and Perugia, and the arterial anatomy of the pancreas was studied. Results A pancreatic branch of the splenic artery running along the superior border of the pancreatic body and tail was observed in 25.93 % of cases. This branch matched the description of the superior horizontal pancreatic artery and, when existing, replaced the pancreatica magna artery. For this reason, we considered the superior horizontal pancreatic artery as a variant of the pancreatica magna artery. Variable in caliber and importance, in most cases the superior horizontal pancreatic artery gave off descending branches that anastomosed with the inferior pancreatic artery. Conclusions A superior horizontal pancreatic artery could be visualized more easily by selective angiography of the S. Mosca Department of Diagnostic Imaging, University of Perugia, Perugia, Italy F. Di Gregorio Department of Bioimaging and Radiological Sciences, Catholic University of Sacro Cuore, Rome, Italy M. Regoli · E. Bertelli (*) Department of Life Sciences, University of Siena, Via Aldo Moro 2, 53100 Siena, Italy e-mail: eugenio.bertelli@unisi.it splenic artery. When coupled with the inferior pancreatic artery, the presence of the superior horizontal pancreatic artery outlined a longitudinally arranged pattern of blood supply of the distal pancreas that should be known. In particular circumstances, extended resections of the gland cutting both longitudinal arteries might jeopardize the surviving of the pancreas remnant. Keywords Pancreas · Blood supply · Pancreatica magna artery · Superior horizontal pancreatic artery Introduction The pancreatic blood supply has received considerable attention over the time due to its high variability. In spite of this, a general agreement on the main arteries supplying the pancreas has been reached even though they show ample variations in incidence, branching pattern and site of origin (Fig. 1). The head of the pancreas is supplied by two anastomotic pancreaticoduodenal arcades joining the superior mesenteric artery with the gastroduodenal artery [3–6]. In addition, the head is also served by the right branch of the dorsal pancreatic artery that anastomoses with the gastroduodenal artery. The dorsal pancreatic artery, in turn, is often the largest pancreatic artery [7]. It arises behind the neck of the pancreas, mostly from the first tract of the hepatic or splenic artery, the celiac trunk or the superior mesenteric artery [7]. The dorsal pancreatic artery gives rise to several minor branches [7, 32] and usually ends close to the inferior edge of the pancreatic neck dividing into two arteries running in opposite directions: the above-mentioned right branch that, forming the prepancreatic arcade and joining the gastroduodenal artery, supplies the head of the pancreas, and a left branch that runs 13 Surg Radiol Anat Fig. 1 a Schematic drawing of the pancreatic blood supply as generally showed in most textbooks and articles. Two pancreaticoduodenal arcades, anterior (APDA) and posterior (PPDA), join the gastroduodenal artery (GD) and the superior mesenteric artery (SM) and supply the head of the pancreas. The dorsal pancreatic artery (DP) descends behind the neck of the gland and divides into two opposite branches: a right one, forming the prepancreatic arcade (PPA) and joining the gastroduodenal artery, and a left one that courses toward the tail of the gland as the inferior pancreatic artery (IP). Two additional arteries are usually shown: the pancreatica magna artery (PM), stemming from the splenic artery (S), penetrates into the body of the pancreas and joins the inferior pancreatic artery, and the caudal pancreatic artery (CP), arising from the last portion of the splenic artery and likewise ending into the inferior pancreatic artery; b schematic drawing of the pancreatic blood supply when a superior horizontal (SH) artery is present. The only difference with a is that the regular pancreatica magna artery is replaced by its transverse variant, the superior horizontal artery. This artery runs nearby the superior margin of the pancreas and gives off several descending branches that usually join the inferior pancreatic artery (IP) toward the tail of the gland along its inferior border. This branch is usually referred to as transverse or inferior pancreatic artery [7]. The body of the pancreas is also supplied by the pancreatica magna artery, which reinforces the inferior pancreatic artery; the tail, in addition of being served by branches of the pancreatica magna artery, also receives few caudal arteries. The pancreatica magna artery and most of the caudal pancreatic arteries originate from the splenic artery. The pancreatica magna artery, also known merely as large pancreatic artery [20] or arteria corporis pancreatis [34], is said to enter the pancreas at the junction of the middle and distal thirds of the gland [35]. Observed with an incidence ranging between 64 and 98 % of cases [8, 31, 34, 35], it descends behind the pancreatic duct and joins the inferior pancreatic artery [20, 22] in about 80 % of cases [31]. In spite of the description carried out by Vandamme [33, 34], the pancreatica magna artery is commonly believed, and accordingly showed, to behave very alike the dorsal pancreatic artery giving off two opposite terminal branches (Fig. 1a) and contributing in this way to extend the course of the inferior pancreatic artery [1, 8, 11, 20, 21, 23, 27, 28, 30, 35]. The inferior pancreatic artery can exist even though the dorsal pancreatic artery does not [24]. In this case, it arises from the gastroduodenal artery, the right gastroepiploic artery or the anterior superior pancreaticoduodenal artery, and crossing anteriorly the pancreatic head, it extends toward the tail of the pancreas as it does when it is a mere branch of the dorsal pancreatic artery. The inferior pancreatic artery comes therefore in at least two variants: a short-type, arising from the dorsal pancreatic artery, and a long-type that, stemming nearby the terminal division of the gastroduodenal artery, runs along the entire length of the gland [2]. This distinction is relevant as the long-type inferior pancreatic artery supplies the head of the pancreas in addition to the body and tail which, in contrast, are the only portions served by the short-type. A careful analysis of a long series of angiographies allowed us to observe with a certain frequency the existence of a vessel arising from the splenic artery that, with a transverse course, often doubled the inferior pancreatic artery (Fig. 1b). When existing, this vessel replaced the pancreatica magna artery, and for this reason, we have considered it as an important morphological variant of the latter artery. In spite of its horizontal course, it differs from the inferior pancreatic artery for its origin, directly from the splenic artery, and for the course located along the superior border of the body and tail of the pancreas. This course closely matches the previously reported superior horizontal pancreatic artery of Popova [25], a vessel that, after a brief appearance in the literature, shortly fell into oblivion. As we believe that the superior horizontal pancreatic artery of Popova may bear clinical importance, we decided to carry out an anatomic study on its general morphology, incidence and course using angiographic archive material; as we consider the superior horizontal pancreatic artery of Popova as a morphological variant of the pancreatica magna artery, we also reviewed briefly the latter artery. 13 Materials and methods For a detailed description of the materials and methods of this research, we refer to a previous publication in this journal [3]. At any rate, we briefly summarize the points of main Surg Radiol Anat Fig. 2 a Selective angiography of the splenic artery; b selective angiography of the celiac trunk; c schematic drawing summarizing the relevant arteries visualized with the angiographic study. A very thin superior horizontal pancreatic artery (SH) supplies the body of the pancreas running leftward close to the superior border of the pancreas and anastomosing with one caudal artery (CP). A dorsal pancreatic artery (DP) is visible issuing from the celiac trunk. The system of the caudal and superior horizontal pancreatic arteries is anastomosed with the inferior pancreatic artery (IP) that marks the inferior border of the pancreas. S splenic artery, CH common hepatic artery, C celiac trunk interest: The present investigation was carried out consulting the angiographic archives of the ex-institutes of Radiology of Siena, Rome (Catholic University) and Perugia. The radiologic examinations of the above-mentioned archives, performed between the years 1983 and 1991, were aimed at studying splenic, intestinal, pancreatic and hepatic pathologies. After having discarded all the examinations which were not suitable for interpreting the vascular anatomy, only 1,015 angiographies were taken into consideration for the anatomic study and included 507 selective angiographies of the superior mesenteric artery, 316 of the celiac trunk, 125 of the common hepatic artery and 67 of the splenic artery. Though the iconography of this investigation has been compiled using the entire collection of angiographies, data on the incidence of the superior horizontal pancreatic artery and of its main features were drawn exclusively from the series of selective angiographies of the splenic artery. The superior horizontal pancreatic artery did not represent as exception to the general variability of the pancreatic blood supply. Actually, it showed a variable degree of development and importance, its diameter ranging from that of a very thin artery (Fig. 2) to about one-third of the splenic artery caliber (Fig. 3). The superior horizontal pancreatic artery always originated directly from the splenic artery (Fig. 3), but in rare instances (3 % of cases) a vessel that could be mistaken for the superior horizontal pancreatic artery appeared as an early branch of the dorsal pancreatic artery (Fig. 4). This vessel was more an anastomotic channel joining the pancreatic branches descending from the splenic artery (the dorsal pancreatic artery with the pancreatica magna artery and the pancreatic magna artery with the caudal pancreatic artery) than an independent artery. With the superior horizontal pancreatic artery, this vessel shared the longitudinal course close to the superior border of the pancreas. However, as in these cases a regular pancreatica magna artery could be identified (Fig. 4), we did consider it merely as a second transverse pancreatic artery. The superior horizontal pancreatic artery supplied variable portions of the distal pancreas. It could appear restricted to the tail of the pancreas (Fig. 5), or it could even extend its territory of competence to part of the body (Fig. 6). In most instances (70.6 % of cases), particularly when it was well developed, the superior horizontal pancreatic artery was co-existing with the inferior pancreatic artery, with which it was often joined through several fine descending branches (Figs. 2, 3, 4, 5), and sometimes (17.6 % of cases), it could end anastomosing with the caudal pancreatic artery (Fig. 2). Less frequently (11.7 % of cases), the Results The superior horizontal pancreatic artery of Popova could be identified in angiographic studies of the celiac artery, especially when combined with those of the superior mesenteric artery. However, due to the overlapping of vessels of the gastric and colic areas, in several cases the identification of this artery was doubtful. Therefore, in order to achieve an estimation of its incidence, we relied only on the selective angiographies of the splenic artery that were much less numerous. In such conditions, a superior horizontal pancreatic artery could be identified in 25.93 % of cases. 13 Surg Radiol Anat Fig. 3 a Selective angiography of the splenic artery; b schematic drawing summarizing the relevant arteries visualized with the angiographic study. The splenic artery (S) gives rise to a superior horizontal artery (SH) that runs leftward giving rise only to fine descending branches (DB), some of them anastomosing with the inferior pancreatic artery (IP) that appears filled with the contrast medium. After giving off the superior horizontal pancreatic artery, the splenic artery does not give rise to any other visible pancreatic branch. The superior horizontal pancreatic artery possibly continues as an epiploic artery (arrowheads, EA) that shows a sinuous course at first ascending and then descending Fig. 4 a Selective angiography of the splenic artery; b schematic drawing summarizing the relevant arteries visualized with the angiographic study. The splenic artery (S) gives rise to four visible pancreatic branches, three of them corresponding to the dorsal pancreatic artery (DP), the pancreatica magna artery (PM) and the caudal pancreatic artery (CP). The fourth branch (1) is small but it helps to visualize the pancreatic silhouette. A fifth branch stems from the inferior splenic branch at the hilus of the spleen (2). The dorsal pancreatic artery descends rightward, and at the inferior margin of the gland, it divides into the usual right and left branches respectively prepancreatic arcade (PPA) and inferior pancreatic artery (IP). From the proximal part of the dorsal pancreatic artery stems, a branch (3) that runs leftward to join the pancreatica magna artery which, in turn, gives rise to a similar branch (4) that joins the caudal pancreatic artery. A second transverse pancreatic artery is formed by the continuity among vessel 3, the pancreatica magna artery, vessel 4 and the caudal pancreatic artery artery appeared as the only artery supplying the distal pancreas with descending branches that did not meet visible inferior pancreatic arteries (Fig. 6). In almost all cases (88.23 % of cases), the superior horizontal pancreatic artery divided in a comb-like fashion giving off several descending branches; they distributed to the pancreas and/or ended anastomosing with the inferior pancreatic artery (Figs. 3, 4, 5). Discussion 13 In our series of angiographies, the superior horizontal pancreatic artery appears in about one case out of four. A selective angiography of the splenic artery is probably the best condition to identify the superior horizontal pancreatic artery due to the lack of overlapping vessels of the gastric or colic areas that appear after injecting the celiac Surg Radiol Anat Fig. 5 a Angiography of the celiac trunk; b angiography of the superior mesenteric artery; c schematic drawing summarizing the relevant arteries visualized with the angiographic study. The celiac artery is affected by a stenosis that determines the enlargement of all the anastomotic pathways joining the mesenteric and the celiac arterial districts, including the pancreaticoduodenal arcades, the prepancreatic arcade, the inferior pancreatic artery and the pancreatic branches of the splenic artery. The combined angiographic approaches allow the identification of the superior horizontal pancreatic artery (SH). The angiography of the celiac trunk shows a large pancreatic branch (SH) issuing from the splenic artery (S) with a leftward course. The vessel runs along the superior margin of the pancreas as demonstrated by the angiography of the superior mesenteric artery showing an inferior pancreatic artery (IP) that marks the inferior border of the gland. In this case, the dorsal pancreatic artery is injected with contrast medium via the superior mesenteric artery. An additional pancreatic branch (1) of the splenic artery, visible only in b, is injected through the inferior pancreatic artery. Also, the left gastroepiploic artery (LGE) is visible only in b, and it is injected through the superior horizontal pancreatic artery and/or the inferior pancreatic artery Fig. 6 a Selective angiography of the splenic artery; b schematic drawing summarizing the relevant arteries visualized with the angiographic study. A very large superior horizontal pancreatic artery (SH) stems from the second third of the splenic artery (S) and supplies the tail and the distal half of the body of the pancreas. The silhouette of the gland is clearly outlined, and though any inferior pancreatic artery is visible, the superior horizontal pancreatic artery can be easily assigned to the superior margin of the pancreas or superior mesenteric arteries. Still, even with a selective angiography, the splenic artery itself can partially eclipse the superior horizontal pancreatic artery sometime hindering the certain identification of the vessel. In other cases, in absence of other radiologic reference points, a superior horizontal pancreatic artery can be mistaken for an inferior pancreatic artery. For instance, it is easier to identify a superior horizontal pancreatic artery when its course is paralleling a regular inferior pancreatic artery, which is known to follow the inferior border of the pancreas. 13 Surg Radiol Anat Fig. 7 a Selective angiography of the splenic artery; b schematic drawing summarizing the relevant arteries visualized with the angiographic study. A pancreatica magna artery (PM) is visible descending from the middle third of the splenic artery (S) and joining the inferior pancreatic artery (IP) at the inferior margin of the pancreas. The course and branching pattern of the pancreatica magna artery are similar to the dorsal pancreatic artery (DP), only placed more distally at the level of the body of the pancreas. Barium (B) remnants from a previous examination are visible in the descending colon By angiography, in absence of a precise reference for the pancreatic margins, it is difficult to assign the course of a transverse vessel to the inferior or the superior border of the gland, particularly when the pancreatic region appears distorted by pathologic processes. It is therefore our feeling that the true anatomic incidence is likely higher than the 25.93 % we estimated, possibly close enough to Evrard’s evaluation [14], which was a little higher than one-third of cases. Clearly, additional studies using computed tomography angiography should help to ascertain a more reliable value, closer to the true anatomic incidence. However, when the superior horizontal pancreatic artery is thin, even computed tomography angiography could fail to spot it. In light of its relatively high incidence, it is puzzling how this vessel has been forgotten after few years from its original description [25] being recalled only by few investigators [14, 17, 29]. This is probably due to the fact that, when existing, the superior horizontal pancreatic artery mostly seems to replace the pancreatica magna artery. It is therefore likely that it has skipped the attention of most researchers as it was considered just as a pancreatica magna artery. It is interesting to note that up to 1930s, the pancreatica magna artery, as we know it today, still seemed to be unknown by most investigators [12, 14, 17, 24, 26], and this very same name was often reserved to the artery that we now refer to as dorsal pancreatic artery [12, 14, 29]. To our knowledge, it is only after Michels’ article on the variations of the splenic artery [20] that the term large pancreatic artery (pancreatica magna artery) became more commonly used to identify a vessel with roughly the same site of origin of the superior horizontal pancreatic artery which, as we said, fell into oblivion. The nomenclature of the pancreatic arteries is a long-lasting point of confusion particularly in what concerns the name pancreatica magna artery [7] that has been used for a long time (up to 1970s) either as 13 a synonym for the dorsal pancreatic artery [9, 10, 13] or as we intend it today to indicate an artery arising from second portion of the splenic artery [1, 20–23, 27, 35]. Indeed, just because the anatomy of the pancreatic arteries is complex and confusing, we do not think that a novel artery should be added to the general scheme that is currently accepted (Fig. 1a). Nevertheless, we believe that within the perimeter of the pancreatica magna artery, a distinction between an artery showing a regular descending course and an artery with the features of the superior horizontal pancreatic artery should be kept in mind. Indeed, when comparing the behavioral and branching pattern of a regular pancreatica magna artery (Fig. 7) with that of a well-developed superior horizontal pancreatic artery (Fig. 3), the differences appear striking and justify reviving an old name. That the pancreatica magna artery can show a various morphology, however, is not so surprising as it may be inferred by the description that Vandamme et al. [33] made of this artery. They affirmed that the pancreatica magna artery lies on the superior border of the pancreas and that it branches in a comb-like fashion giving off small descending rami that enters the substance of the gland contributing to the formation of the inferior pancreatic artery: a description more fitting to the superior horizontal pancreatic artery than to the commonly acknowledged pancreatica magna artery. Actually, a pancreatic magna artery with the features of a superior horizontal pancreatic artery can be easily observed in anatomic specimens injected with contrast medium by several authors [1, 21, 34]. Though not sufficiently underlined, the variable morphology of the pancreatica magna artery has been admitted by other authors that observed a vertical course in 96 % of cases versus a transverse one in 4 % of cases [31]; however, if we assume the artery with a transverse course having the features of a superior horizontal pancreatic artery, the incidence reported by Toni et al. Surg Radiol Anat [31] appears much lower than ours or the one observed by Evrard [14]. The difference in the statistical surveys can be expected as Toni et al.’s analysis of the pancreatic arteries was carried out using exclusively standard angiographies of the celiac artery [31] that, as discussed earlier, can be more troublesome for the identification of the superior horizontal pancreatic artery. The presence of the superior horizontal pancreatic artery coupled with the inferior pancreatic artery (the most frequent occurrence) outlines a previously acknowledged longitudinally arranged arterial blood supply pattern of the body and tail of the pancreas [16, 18, 19]. According to Mellière [19], an arterial arrangement like this, where the distal part of the pancreas is served only by transverse arteries that do not anastomose with the splenic artery, occurs in ¼ of cases, which is roughly the same incidence that we determined for the superior horizontal pancreatic artery. When such an arterial pattern exists, an extended pancreatic resection leaving the distal part of the body and tail of the pancreas is virtually impossible. Conflict of interest The authors declare that they have no conflict of interest. References 1. Belli L, De Marzo V, Tiberio G, Morisi M (1958) Contributo allo studio della circolazione arteriosa intrapancreatica. Biol Lat 11:375–394 2. Bertelli E (2004) Arterial blood supply of the pancreas. In: Skandalakis JE, Colborn GL, Weidman TA, Foster RS, Kingsnorth AN, Skanadaliks LJ, Skandalakis PN, Mirilas PS (eds) Skandalakis surgical anatomy. The embryologic and anatomic basis of modern surgery. Vol 1, PMP, Athens pp 1185–1191 3. Bertelli E, Di Gregorio F, Bertelli L, Mosca S (1995) The arterial blood supply of the pancreas: a review. I. The superior pancreatico-duodenal and the anterior superior pancreatico-duodenal arteries. An anatomical and radiological study. Surg Radiol Anat 17:97–106 4. Bertelli E, Di Gregorio F, Bertelli L, Civeli L, Mosca S (1996) The arterial blood supply of the pancreas. II. The posterior superior pancreaticoduodenal artery. An anatomical and radiological study. Surg Radiol Anat 18:1–9 5. Bertelli E, Di Gregorio F, Bertelli L, Civeli L, Mosca S (1996) The arterial blood supply of the pancreas. III. The inferior pancreaticoduodenal artery. An anatomical and radiological study. Surg Radiol Anat 18:67–74 6. Bertelli E, Di Gregorio F, Bertelli L, Orazioli D, Bastianini A (1997) The arterial blood supply of the pancreas. IV. The anterior inferior and posterior pancreaticoduodenal arteries, and minor sources of blood supply for the head of the pancreas. An anatomical and radiological study. Surg Radiol Anat 19:203–212 7. Bertelli E, Di Gregorio F, Mosca S, Bastianini A (1998) The arterial blood supply of the pancreas. V. The dorsal pancreatic artery. An anatomical and radiological study. Surg Radiol Anat 20:445–452 8. Bolognese A, Di Giorgio A, Stipa V (1979) Arterial vascularization of the pancreas. Anatomical findings by means of vascular injection of plastic material. Surg Italy 9:346–351 9. Bouchet Y, Martin R (1961) Considérations sur l’artère pancreatica magna ou pancréatique dorsale. CR Ass Anat 111:174–179 10. Bourret P, Viale G (1953) Les artères parenchymateuses du pancréas. CR Ass Anat 40:467–471 11. Busnardo AC, DiDio LJA, Thomford NR (1988) Anatomosurgical segments of the human pancreas. Surg Radiol Anat 10:77–82 12. Del Campo JC (1931) Circulación del duodeno. Anales Facultad Med Montevideo 16:1–27 13. Delagrange AB, Barbin JY (1966) Contribution a l’étude de la vascularisation artèriélle du pancréas. CR Ass Anat 135:297–306 14.Evrard HL (1932) Les artères du duodénum et du pancréas. These #640, Paris 15.Gilroy AM, MacPherson BR, Ross LM (2012) Atlas of anatomy, 2nd edn. Thieme Medical Publisher, New York 16. Hentshel M (1965) Pankreas-Anatomie. Langenbecks Arch Klin Chir 313:233–242 17. Kirk E (1931) Untersuchungen über die gröbere und feinere topographische Verteilung der Arterien, Venen und Ausführungsgänge in der menschlichen Bauchspeicheldrüse. Z Ges Anat 94:822–875 18. Martin R, Bouchet Y, Gouppie G (1961) Considérations sur l’artère splénique et ses branches pancréatiques. C R Ass Anat 113:513–529 19. Mellière D (1968) Variations des artères hépatique et du carrefour pancréatique. J Chir 95:5–42 20. Michels NA (1942) The variational anatomy of the splenic artery. Am J Anat 70:21–72 21. Moretti S (1965) Studio anatomo-radiografico del circolo arterioso pancreatico. Radiol Med 51:1–16 22.Nebesar RA, Kornblith PL, Pollard JJ, Michels NA (1969) Celiac and superior mesenteric arteries. A correlation of angiograms and dissections. Little Brown, Boston 23. Peri G, Veralli E, Trivellini G (1969) La vascolarizzazione del pancreas. Arch It Chir 95:287–300 24. Pitzorno M (1920) Morfologia delle arterie del pancreas. Arch Ital Anat Embriol 18:1–48 25. Popova AV (1910) Contribution a l’étude de la distribution du système artériel dans le pancréas des enfants nés avant term. Arch Soc Sci Med Biol Montpellier 15:139–144 26. Branco Rio, da Silva P (1912) Essai sur l’anatomie et la médecine opératoire du tronc cœliaque et de ses branches de l’artère hépatique en particulier. Steinheil, Paris 27. Rossotto P, Motta G, Azzena GF, Ferraris R (1967) Ricerche anatomiche sulla vascolarizzazione arteriosa del pancreas. Min Chir 22:101–104 28. Ruzicka FF, Rankin RS (1977) Normal arterial anatomy of the abdominal viscera. CRC Crit Rev Diagn Imaging 9:337–385 29. Sobotta J (1914) Anatomie der bauchspeicheldrüse (pankreas). Bardeleben Handbuch der Anatomie des Menschen 6:1–62 30.Thomford NR, Chandnani PC, Taha AM, Chablani VN, Busnardo AC (1986) Anatomic characteristics of the pancreatic arteries. Radiologic observations and their clinical significance. Am J Surg 151:690–693 31.Toni R, Favero L, Mosca S, Ricci S, Roversi R, Vezzadini P (1988) Quantitative clinical anatomy of the pancreatic arteries by selective celiac angiography. Surg Radiol Anat 10:53–60 32.Tsutsumi M, Arakawa T, Terashima T, Aizawa Y, Kageyama I, Kumaki K, Miki A (2013) Morphological analysis of the branches of the dorsal pancreatic artery and their clinical significance. Clin Anat. doi:10.1002/ca.22331 33. Vandamme JP, Van der Schueren G, Bonte J (1967) Vascularization du pancreas: proposition de nomenclature P.N.A. et angioarchitecture des ilots. CR Ass Anat 137:1184–1189 34. Vandamme JPJ, Bonte J (1986) Systematization of the arteries in the splenic hilus. Acta Anat 125:217–224 35. Woodburne RT, Olsen LL (1951) The arteries of the pancreas. Anat Rec 111:255–270 13