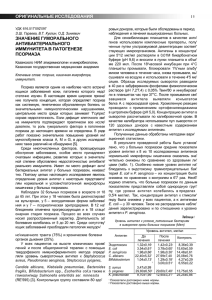
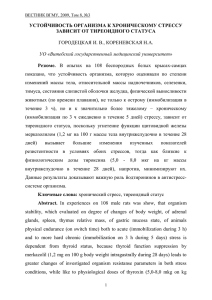
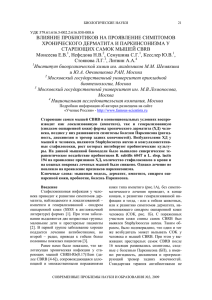
Second problem: Skin and Soft Tissue Infections The patient was a 45-year-old male who was in his usual state of good health when he awoke at 3am with pain in the lateral aspect of his left calf. He looked at his calf and thought that the pain was due to an ingrown hair and went back to sleep. At 10am, he expressed a small amount of pus from the ingrown hair. Over the next 8h, the patient developed an area of cellulitis on the lateral aspect of the calf of approximately 5 to 10 cm. At that time, a small amount of pus was again extended from just below the knee to just above the ankle. The patient visited his physician. His vital signs at that visit, including pulse, respirations, blood pressure, and temperature, were all within normal limits. Physical exam was significant for an area of obvious fluctuant. No lymphadenopathy was observed. The central area of the cellulitis, near the area that the patient described as where the ingrown hair had been, was punctured three tirnes, but no pus was drained. The patient was referred to the surgery service. The surgeons examined the patient and said they would follow him. The patient was given 2g ceftriaxone IM and begun on oral cephalexin. The patient returned to the surgical clinic 48 hours later with an obvious area of fl uctuance in the center of the area of cellulitis. Over the preceding 48 hours, the patient reported low-grade fevers. Approximately 1 ml of pus was aspirated and was sent for Gram stain and culture (Fig. 36.1 and 36.2). When pus was aspirated from the lesion, the surgeon decided to excise and drain the lesion (Fig. 36.3). —------------------------------------------------------------------------------------------------------------------------- The Aim: ● Knowledge of the microorganisms involved into the Skin, Soft tissue, Bone & Joint infections: microbiology, pathogenesis, epidemiology, laboratory diagnosis, treatment, prevention and control The plan of self-directed learning: ● ● Bacteria (S. aureus, S. pyogenes, H influenza, E. aerogenes, M. tuberculosis): microbiology, pathogenesis, epidemiology, laboratory diagnosis, treatment, prevention and control . Fungi (B. dermatitidis, C. neoformans): mycology, pathogenesis, epidemiology, laboratory diagnosis, treatment, prevention and control What is the organism most likely causing this patient’sinfection? What other type of infections does this organism How do you think he became infected with this organism? Why were incision and drainage necessary to treat thisinfection? Why would antimicrobial agents alone not be 1. Describe what you observed in Fig. 36.1 and 36.2. The organism is catalase and coagulase positive. What organism was causing his infection? 2. Why were incision and drainage necessary to treat this infection? Why would antimicrobial agents alone not be effective in treatment of this infection? 3. Susceptibility results for this organism are seen in Fig. 36.4. How do you interpret these susceptibility results? Explain the likely reasons for the results seen with drugs 2 and 4. How do results of the testing of drug 2 explain the progression of his infection despite a large intramuscular dose of ceftriaxone followed by oral cephalexin? Also explain the fi ndings for drugs 7 and 8. How should the isolate infecting this patient be treated? 4. What test is being used to test vancomycin (drug 5)? Why is this test being used and what does it show? 5. What virulence factor is particularly associated with skin and soft tissue infections (SSTIs)? Explain its mechanism of action. This virulence factor and this type of antibiogram are associated with a particular strain of this organism. Briefl y discuss the evolving epidemiology of this strain. 6 What infection control precautions would be necessary for this patient? What are some of the potential unintended consequences of hospitalized patients who are colonized with this organism? 7. Why are these organisms viewed as a global threat? CASE DISCUSSION 1. The finding of Gram-positive cocci in clusters on Gram stain is consistent with staphylococci. The fi nding of a yellowish colony that is beta-hemolytic on 5% sheep blood agar is consistent with Staphylococcus aureus . The staphylococci are divided into two groups based on the biochemical test called the coagulase test; S. aureus is positive, while a group of >30 other staphylococcal species are negative. This group of organisms is referred to as the coagulase-negative staphylococci (CoNS). Three of the CoNS species are frequently encountered clinically. Staphylococcus epidermidis can infect implanted foreign bodies, such as pacemak- ers, cerebrospinal fl uid shunts used to treat hydrocephalus, intravascular catheters, and artifi cial joints. Staphylococcus lugdunensis has been associated with skin and soft tissue infections (SSTIs) as well as native valve endocarditis. Although S. lugdunensis can cause SSTIs, it is less common than S. aureus . The other frequently encountered CoNS species is Staphylococcus saprophyticus , which causes urinary infections primarily in young, sexually active women. The isolate recovered from this patient was coagulase positive and was identifi ed as S. aureus . The patient’s infection began as a folliculitis at the site of the ingrown hair, progressed to a cellulitis, and ultimately evolved into an abscess. Approximately 20% of adults are chronic nasal carriers of S. aureus , while an additional 60% may carry the organism intermittently. From the nose, the skin can become colonized. Studies have shown intermittent skin carriage rates as high as 40%, although most studies target the skin carriage rate at 10 to 15%. In all likelihood this individual’s initial folliculitis was a result of the infecting S. aureus coming from skin colonization. Manipulation of the skin resulted in the spread of the organism to the dermis, leading to cellulitis and abscess formation. 2. The standard of care for an abscess is 2-fold: incision and drainage (Fig. 36.3) and antimicrobial therapy. The reason why antibiotics alone would not be suffi cient is that abscess formation results in a loss of blood fl ow to the center of the infected area (the abscess). As a result, antibiotic levels in the center of the abscess would be low or, in a large abscess, completely absent, allowing the survival of the infecting organisms present there. Incision and drainage removes a large number of organisms and reduces the infected area, making penetration of much higher levels of antimicrobial agents to the infected tissue and killing of the infecting organism more likely. Staphylococcus 3. The susceptibility test that was performed on this patient is a disk diffusion test for seven drugs and an E-test for one drug. The basis for disk diffusion susceptibility testing is described in the introductory chapter of this text, and the reader is referred there for further details. The antibiogram for this organism is as follows: Drug 1: trimethoprim-sulfamethoxazole, to which the organism is susceptible Drug 2: cefoxitin, to which the organism is resistant Drug 3: doxycycline, to which the organism is susceptible Drug 4: penicillin G, to which the organism is resistant Drug 5: vancomycin with an MIC of 2 μg/ml by E-test (see answer 3 for more details) Drug 6: gentamicin, to which the organism is susceptible Drug 7: clindamycin, to which the organism is susceptible Drug 8: erythromycin, to which the organism is resistant This S. aureus strain is expressing two different resistance mechanisms against the β -lactam drugs. One is evidenced by its resistance to penicillin G. This resistance is due to the organism’s ability to produce an enzyme, β -lactamase, that degrades the β -lactam ring of penicillin G, rendering this and the related widely used antimicrobials ampicillin, amoxicillin, and piperacillin inactive. Approximately 90 to 95% of S. aureus strains produce a β -lactamase that is encoded on the bacterial chromosome. Almost as soon as penicillin G was put into widespread therapeutic use, recognition of S. aureus strains resistant to penicillin G by virtue of β -lactamase production emerged. New agents including penicillinase-stable penicillins (oxacillin, nafcillin, and the oral agent dicloxacillin); first-, second-, and third-generation cephalosporins; and carbapenems were developed over the following decades. A characteristic all these drugs shared was that they were relatively stable in the presence of β -lactamase-producing S. aureus . However, a second resistance mechanism to β -lactam drugs soon emerged. The presence of this resistance is predicted by the cefoxitin result. Although cefoxitin is not a drug that is used to treat S. aureus infections, S. aureus strains expressing cefoxitin resistance predictably have alteration of a specific penicillin-binding protein, PBP2. The altered penicillin-binding protein, PBP2a, is encoded by mecA . All β -lactam antimicrobials have significantly reduced affinity for PBP2a relative to PBP2. This altered affinity is the basis for what we call methicillin resistance in S. aureus . This term is obviously a bit of a misnomer since this PBP alteration confers resistance to all β -lactam drugs, just not methicillin. The reason the term “methicillin-resistant S. aureus ,” or MRSA, became widespread is that methicillin was the drug used to treat serious S. aureus infections when this resistance was first encountered. It is critical to remember that no β -lactam antimicrobial has clinical efficacy against MRSA with the exception of a newly developed cephalosporin, ceftaroline, although some β -lactams may appear to have activity against S. aureus in vitro . The only other antimicrobial to which this isolate is resistant is erythromycin. If the placements of the clindamycin (disk 7) and erythromycin (disk 8) disks are closely examined, it should be noted that they are closer together than the other disks in order to determine whether there is formation of a D-shaped zone of inhibition around the clinGilligan_Sec4_255-306.indd 264 7/24/14 11:44 AM damycin. The D-zone occurs when erythromycin induces the production of an rRNA methylase encoded by the erm gene. Expression of this methylase can be either constitutive (always on) or inducible (on only in the presence of an inducer such as erythromycin). erm -specific methylation of the rRNA results in both erythromycin and clindamycin resistance. The D-zone test is assessing whether the inducible form of erm is present. The bacteria growing closest to the erythromycin disk are in the presence of an inducer, and therefore will be resistant to clindamycin; this resistance causes a “flattening” of the zone of inhibition in the area between the two disks, creating a characteristic D-shaped zone around the clindamycin disk (Fig. 36.3). If the constitutive form of erm was present, the organism would test as resistant to clindamycin independent of the presence of erythromycin. Clinical failures of clindamycin therapy for infections due to S. aureus strains with inducible erm genes are well documented in the literature. Mild SSTIs can be treated with oral antimicrobials. Because his isolate was resistant by virtue of altered PBPs to both of the drugs he was given initially, ceftriaxone and cephalexin (an oral cephalosporin), this patient next was given oral clindamycin. Some studies suggest that incision and drainage is all that is necessary to clear the infection, but the physician was being cautious. 4. Vancomycin is a key drug in treating MRSA infections, particularly severe ones as seen in this patient. Vancomycin (drug 5) is being tested using a special antimicrobialimpregnated strip called an E-test. The strip is designed to release a gradient of a specific antimicrobial agent into the agar. The point where the elliptical zone of bacterial growth inhibition (thus the name “E-test”) meets the strip determines the MIC of the antimicrobial for the organism being tested. The vancomycin MIC is 2 μg/ml, which is at the upper level of susceptibility for this organism. Strains with vancomycin MICs of 4 or 8 μg/ml are referred to as vancomycin-intermediate S. aureus , or VISA, and are more likely to result in treatment failures. VISA strains are not reliably detected by disk diffusion techniques; thus the need for a MIC technique. The reduced susceptibility of VISA isolates is due to a thickening of the cell wall, resulting in “trapping” of vancomycin, a large, highly charged molecule. VISA strains should not be confused with vancomycin-resistant S. aureus , or VRSA. VRSA strains are still quite rare worldwide. Their resistance is due to the acquisition of the vanA gene from Enterococcus faecium . VRSA strains have high-level vancomycin resistance (MICs of 16 to ≥128 μg/ml). 5. Panton-Valentine leukocidin is a virulence factor that is specifically associated with SSTIs. It is a cytolytic pore-forming hexameric protein that can lyse a variety of cell types. It has particular affinity for polymorphonuclear cells and macrophages (thus the name “leukocidin”). With increasing frequency, S. aureus strains with a specific molecular signature have been documented to be responsible for significant SSTIs causing individuals to seek care in emergency departments. These strains are called community-associated MRSA, or CA-MRSA. CA-MRSA strains carry the lukS-PV and lukF-PV genes encoding PantonValentin leukocidin and a small staphylococcal chromosomal cassette (SCC mec type IV) that harbors mecA . Among CA-MRSA isolates, a specific pulsed-field gel electrophoresis pattern Gilligan_Sec4_255-306.indd 265 7/24/14 11:44 AM