Premalignant and Malignant Lesions of the Heterotopic Pancreas in the Esophagus
advertisement

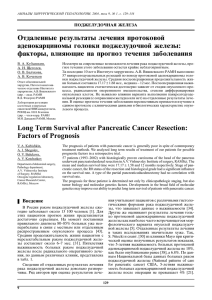
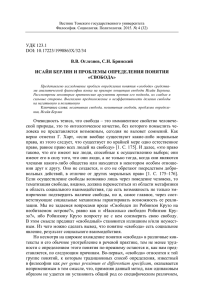
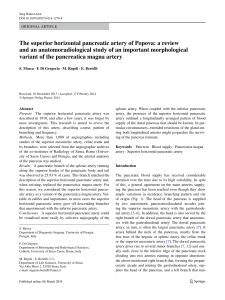
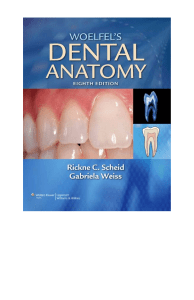
case report Available from: URL: http://www.jgld.ro/2015/2/19.html DOI: http://dx.doi.org/10.15403/jgld.2014.1121.242.uly Premalignant and Malignant Lesions of the Heterotopic Pancreas in the Esophagus: a Case Report and Review of the Literature Jan Ulrych1, Vladimir Fryba1, Helena Skalova2, Zdenek Krska1, Tomas Krechler3, David Zogala4 1) 1st Department of Surgery - Department of Abdominal, Thoracic Surgery and Traumatology; 2) Institute of Pathology; 3) 4th Department of Medicine - Department of Gastroenterology and Hepatology; 4) Institute of Nuclear Medicine; First Faculty of Medicine, Charles University in Prague and General University Hospital in Prague, Prague, Czech Republic Address for correspondence: Jan Ulrych MD 1st Department of Surgery First Faculty of Medicine, Charles University in Prague General University Hospital in Prague U Nemocnice 2, 128 08, Prague 2, Czech Republic Jan.Ulrych@vfn.cz, Received: 06.03.2015 Accepted: 03.04.2015 Abstract Heterotopic pancreas is a congenital pathology of the gastrointestinal tract, particularly rare in the esophagus. Both symptomatology and findings during preoperative examinations are non-specific and therefore do not often lead to an accurate diagnosis, which is usually revealed only by histopathological assessment of a resected specimen. We report an unusual case of a patient suffering from severe dysphagia caused by heterotopic pancreas in the distal esophagus with chronic inflammation and foci of premalignant changes. This article also reviews 14 adult cases of heterotopic pancreas in the esophagus previously reported in the literature, with the aim of determining the clinical features of this disease and possible complications including rare premalignant lesions and malignant transformation. Especially with regard to those complications, we suggest that both symptomatic and incidentally found asymptomatic lesions should be resected. Key words: heterotopic pancreas – esophagus – pancreatic intraepithelial neoplasia – submucosal esophageal tumor. Abbreviations: AFP: alpha-fetoprotein; CA 19.9: cancer antigen 19.9; CEA: carcinoembryonic antigen; CYFRA: cytokeratin 19 fragment; FDG: fluorodeoxyglucose; GERD: gastroesophageal reflux disease; GIST: gastrointestinal stromal tumor; IPMN: intraductal papillary mucinous neoplasia; PanIN: pancreatic intraepithelial neoplasia; PSA: prostate specific antigen; SCCA: squamous cell carcinoma antigen. Introduction Heterotopic pancreas is a rare condition defined as the occurrence of pancreatic tissue in an abnormal location without any anatomic or vascular continuity with orthotopic pancreas [1]. Heterotopic pancreas can arise in any part of the gastrointestinal tract, most frequently in the stomach, duodenum or jejunum [2]. Up to now, there have been only 14 cases of heterotopic pancreas in the esophagus in adult patients documented in the literature [3-16]. Ectopic tissue is usually discovered incidentally or may become symptomatic because of obstruction caused by enlargement due to inflammation, bleeding or malignant transformation [3, 6, 7]. A malignant tumor arising in the heterotopic pancreas is an extremely rare event described in 28 cases in the gastroduodenal region and in a few cases in other locations [17-20], including 2 in the esophagus [5, 7]. Premalignant lesions, namely in the form of pancreatic intraepithelial neoplasia (PanIN), are found not only adjacent to malignant tumors, but also in patients without invasive carcinoma. We report an unusual case of a patient suffering from severe dysphagia caused by heterotopic pancreas in the distal esophagus with chronic inflammation and foci of premalignant changes. Case report An obese 34-year-old man was admitted to the inpatient department with severe dysphagia. His medical history included only a cholecystectomy 8 years ago. He confessed to smoking 10 cigarettes per day and occasional alcohol drinking. For several years, he had suffered from dyspepsia, which had been in the last 3 months complicated by progressive dysphagia, at first for solid food, later for liquid, together with odynophagia and J Gastrointestin Liver Dis, June 2015 Vol. 24 No 2: 235-239 236 Ulrych et al regurgitation. He complained about weakness and weight loss of 10 kg in the last 2 months. Physical examination, hematological, biochemical and tumor marker (AFP, CEA, CA19.9, CYFRA, PSA, beta2-microglobulin, SCCA) tests were within normal limits. Esophagogastroduodenoscopy showed a narrowing of the lower esophagus due to a protruding mass lesion covered by normal mucosa. Endoscopic mucosal biopsy revealed only mild inflammation without neoplastic or any other pathological changes. Endoscopic ultrasonography failed because the endoscope could not pass around the protruding mass. Positron emission tomography and computed tomography (PET-CT) revealed a large hypermetabolic tumor mass 100x50x40 mm in size, located in the dorsal wall of the lower esophagus, without any distal lymph nodal involvement (Fig. 1). Contrastenhanced CT demonstrated a tumor mass arising from the lower esophagus without any ingrowth to pericardium or pleura. Bronchoscopy did not discover any remarkable changes. Fig. 2. Tissue mass resected from the lower esophagus. Fig. 3. Heterotopic pancreas with characteristic lobular structure and hyperplasia of the ducts, surrounded by esophageal muscular layer (lower right) (H&E x40). Fig. 1. Axial fused fluorodeoxyglucose PET/CT image shows a soft tissue mass with high FDG uptake in the lower posterior mediastinum. After multi-disciplinary discussion the patient underwent surgery of this symptomatic, histologically non-verified mass lesion in the lower esophagus. Left-side posterolateral thoracotomy was performed. Intraoperative exploration showed a large tumor arising from the wall of the distal esophagus and adhesions to the mediastinal pleura, pericardium, pulmonal ligament and descending aorta. This regionally advanced but resectable tumor was removed with distal esophagus resection; afterwards primary anastomosis and partial fundoplication were carried out. Intraoperative biopsy of the unevenly shaped specimen 50x40x20 mm in size (Fig. 2) had a strikingly unexpected outcome: heterotopic pancreatic tissue. Histopathological examination showed characteristic lobulated pancreatic tissue encompassing acini, minute Langerhans islets and many cystically dilated irregular ducts (Fig. 3), that according to Heinrich’s classification matched type I (Table I). Pancreatic tissue was partially changed by marked chronic inflammation (Fig. 4) with suppurative destruction of several larger ducts. Ductular epithelium focally evidenced marked reactive changes and papillary proliferation, morphologically compatible with pancreatic intraepithelial neoplasia of mild and moderate grade (PanIN 1-2). Bundles of esophageal smooth muscle layer were seen at the periphery of the specimen. J Gastrointestin Liver Dis, June 2015 Vol. 24 No 2: 235-239 Fig. 4. Chronic pancreatitis with fibrosis and a dilated larger duct with reactive epithelial papillary proliferation that is morphologically compatible with PanIN 1 and 2 (lower left) and hyperplasia of small ducts (H&E x100). The postoperative course was uneventful, and after three months, the patient is free from symptoms and remains under the supervision of a gastroenterologist. Discussion Heterotopic pancreas is a congenital anomaly, defined as the presence of pancreatic tissue outside its normal location without anatomic, neural and vascular connection with the orthotopic pancreas [1, 2]. Other terms such as ectopic, Heterotopic pancreas in the esophagus 237 Table I. Heinrich´s classification of the heterotopic pancreas. Type Histopathological characteristics Type I ducts, acini and endocrine islets similar to those seen in normal pancreatic tissue Type II large number of acini, a few ducts and no islets Type III numerous ducts, a few acini and no islets Type IV – modification by Gaspar-Fuentes entirely endocrine islets with no exocrine pancreatic tissue aberrant or accessory pancreas have been used in the relevant literature [21]. Presumably, it results from separation of small parts of pancreatic tissue during the process of foregut rotation and the fusion of the dorsal and ventral pancreatic buds [2, 22]. The first case of heterotopic pancreas was reported by Schultz in 1727, but the first histological confirmation was described by Klob in 1859 [23]. Generally, the prevalence of ectopic pancreas is low. It is discovered in 0.5 – 13.7% of autopsies and in approximately 1 of 500 operations of the upper abdomen [24]. Most frequently, it is found in the stomach (25-38%), duodenum (17-21%) and jejunum (15-21%), although it can occur in any part of the gastrointestinal tract and, moreover, in the abdominal cavity, lung or mediastinum [22, 25-27]. In the gastrointestinal tract, it is most frequently located only in submucosa (54%), less frequently in submucosa and muscularis propria together (23%), only muscularis propria (8%), subserosa (11%) and, rarely, in the whole wall (4%) [28]. Histological structure was originally classified by Heinrich with later modification by Gaspar-Fuentes et al. (Table I) [29, 30]. Most patients are asymptomatic and heterotopic pancreas is found incidentally. Some patients may present with various non-specific symptoms that depend on the site of the lesion and type of complication. Preoperative diagnostic process is usually unsuccessful, because all the imaging techniques typically show a tumor mass in the wall of gastrointestinal tract without any specific sign and endoscopic biopsy commonly contains only isolated normal or mildly inflamed mucosa, which covers the mass. Before surgical resection, the lesion is frequently misdiagnosed as one of the most common submucosal tumors, gastrointestinal stromal tumor (GIST) or leiomyoma [2, 6, 31]. In many cases, the correct diagnosis is not determined until the histopathological examination of the resected specimen [6, 10-14, 24]. The heterotopic pancreas is susceptible to the same pathological changes that occur in a normal pancreas, such as acute or chronic inflammation with fibrosis and pseudocyst formation [2, 6, 11, 32]. Moreover, premalignant changes seem to occur with the same incidence in heterotopic and orthotopic pancreas. In both types of pancreatic tissue, the most frequent precursor of an invasive carcinoma is PanIN, a noninvasive flat or papillary epithelial proliferation with different degree of architectural and cytological atypia [33, 34]. Progression from mild changes (PanIN 1) to higher dysplasia (PanIN 2, 3) and finally adenocarcinoma is accompanied by gradual accumulation of genetic abnormalities. Zhang et al. studied a small group of patients with synchronous ductal adenocarcinoma of orthotopic pancreas and pancreatic heterotopia, where they found PanIN of variable grade in all cases. Interestingly, both adenocarcinomas and PanINs had a similar pattern of p53, cyclin D1 and p16 expression in all cases and the same K-ras codon 12 mutation in half of the cases [35]. In heterotopic pancreas, only single cases of another precursor lesion, intraductal papillary mucinous neoplasia (IPMN) have been documented, including one in the esophagus [14, 36]. Malignant transformation is an extremely rare event described in 18 cases in the stomach, 10 cases in the duodenum and in a few cases in other locations, such as the esophagus, jejunum, ampulla of Vater, spleen, mesocolon, liver and rectum [20]. Most of them were ductal adenocarcinomas; other types such as acinar cell carcinoma, mucinous cystadenocarcinoma, solid pseudopapillary neoplasia, anaplastic carcinoma and Table II. Previously reported cases of the heterotopic pancreas in the esophagus in adults. Case Gender Age (years) Location in Esophagus Symptomatology Associated anomalies Neoplasia Ref. 1. M 43 Distal third Hematemesis None No 3 2. M 25 Middle third Vomiting, epigastric discomfort Congenital cyst No 4 3. M 60 Distal third Dysphagia, epigastric pain, weight loss None Adenoca 5 4. F 47 Distal third Dysphagia, epigastric pain, weight loss None No 6 5. M 45 Distal third Dysphagia None Anaplastca 7 6. F 24 Distal third Nausea, vomiting, fever None No 8 7. M 52 Distal third Dysphagia None No 9 8. F 41 Distal third GERD, dysphagia, epigastric pain, weight loss None No 10 9. F 26 Distal third Epigastric pain, nausea None No 11 10. M 63 Middle third Asymptomatic None No 12 11. F 38 Distal third GERD, epigastric pain None No 13 12. F 58 Distal third Dysphagia None IPMN 14 13. M 25 Distal third Epigastric pain None No 15 14. F 73 Distal third Epigastric pain, vomiting None No 16 F = female, M = male, GERD = gastroesophageal reflux disease, Ref. = references, Adenoca = adenocarcinoma, Anaplastca = anaplastic carcinoma, IPMN = intraductal papillary mucinous neoplasia J Gastrointestin Liver Dis, June 2015 Vol. 24 No 2: 235-239 238 neuroendocrine adenocarcinoma appeared in single cases [20]. An extensive sampling of such tumors is always necessary to evaluate the origin in the ectopic tissue and exclude the possibility of coincidental lesions. Up to date, there have been only 14 cases of esophageal heterotopic pancreas in adults reported in the literature with equal incidence between males and females (Table II) [3-16]. Most patients suffered from dysphagia and epigastric pain, sometimes accompanied by signs of gastroesophageal reflux, nausea and rarely hematemesis. In the vast majority of patients including our case, the heterotopic tissue was located in the distal third of the esophagus. Related congenital esophageal abnormalities, sometimes found in children, are exceptional in adults [4]. In our patient, chronic pancreatitis might be the reason for the recent enlargement and escalation of symptoms. The described finding of PanIN alerts to an increased risk of malignant transformation [33-35], that has been so far reported only in 2 patients with esophageal heterotopic pancreas, once in the form of ductal adenocarcinoma, once in the form of anaplastic carcinoma (Table II). Conclusion Cases of heterotopic pancreas located in the wall of the esophagus are extremely rare. Accurate preoperative diagnosis is difficult and often incorrect and the lesion is frequently misdiagnosed as a tumor. Treatment differs according to the clinical course. Symptomatic lesions are usually resected, which enables histopathological examination of the specimen. Conservative treatment can be considered in small asymptomatic lesions but always carries the risk of underestimation regarding its nature and biological behavior. The equal incidence of precancerous lesions in heterotopic and orthotopic pancreas is a warning of the possibility of malignant transformation, although it seems to be an exceptional event. Considering all potential complications, we suggest that both symptomatic and incidentally found asymptomatic lesions should be resected. Conflicts of interest: No conflict to declare. Authors´ contribution: J.U., V.F., H.Sk. designed the report and collected the patient´s clinical data; Z.K. performed the operation; T.K. performed the preoperative assessment and diagnosis; D.Z. dealt with the figures. References 1. Wlaź J, Mądro A, Kaźmierak W, Celiński K, Słomka M. Pancreatic and gastric heterotopy in the gastrointestinal tract. Postepy Hig Med Dosw (Online) 2014; 68: 1069-1075. 2. Trifan A, Târcoveanu E, Danciu M, Huţanaşu C, Cojocariu C, Stanciu C. Gastric heterotopic pancreas: an unusual case and review of the literature. J Gastrointestin Liver Dis 2012; 21: 209-212. 3. Razi MD. Ectopic pancreatic tissue of esophagus with massive upper gastrointestinal bleeding. Arch Surg 1966; 92: 101-104. doi: 10.1001/ archsurg.1966.01320190103024 J Gastrointestin Liver Dis, June 2015 Vol. 24 No 2: 235-239 Ulrych et al 4. Salo JA, Dlouhy M, Virtanen I. Congenital cyst and heterotopic pancreatic tissue in the oesophagus. Ann Chir Gynaecol 1993; 82: 263-265. 5. Guillou L, Nordback P, Gerber C, Schneider RP. Ductal adenocarcinoma arising in a heterotopic pancreas situated in a hiatal hernia. Arch Pathol Lab Med 1994; 118: 568-571. 6. Noffsinger AE, Hyams DM, Fenoglio-Preiser CM. Esophageal heterotopic pancreas presenting as an inflammatory mass. Dig Dis Sci 1995; 40: 2373-2379. doi: 10.1007/BF02063240 7. Roshe J, Del Buono E, Domenico D, Colturi TJ. Anaplastic carcinoma arising in ectopic pancreas located in the distal esophagus. J Clin Gastroenterol 1996; 22: 242-244. 8. Temes RT, Menen MJ, Davis MS, Pett SB Jr, Wernly JA. Heterotopic pancreas of the esophagus masquerading as Boerhaave’s syndrome. Ann Thorac Surg 2000; 69: 259-261. doi: 10.1016/S0003-4975(99)01223-0 9. Shalaby M, Kochman ML, Lichtenstein GR. Heterotopic pancreas presenting as dysphagia. Am J Gastroenterol 2002; 97: 1046-1049. doi: 10.1111/j.1572-0241.2002.05627.x 10. Rodriguez FJ, Abraham SC, Allen MS, Sebo TJ. Fine-needle aspiration cytology findings from a case of pancreatic heterotopia at the gastroesophageal junction. Diagn Cytopathol 2004; 31: 175-179. doi: 10.1002/dc.20066 11. Gananadha S, Hunt DR. A unique case of pancreatitis and retention cyst in esophageal heterotopic pancreas. Surg Laparosc Endosc Percutan Tech 2005; 15: 345-347. 12. Goto J, Ohashi S, Okamura S, et al. Heterotopic pancreas in the esophagus diagnosed by EUS-guided FNA. Gastrointest Endosc 2005; 62: 812-814. doi: 10.1016/j.gie.2005.04.031 13. Garn T, Hallenscheidt T, Schumacher B, Krämling HJ. Tumor of the esophagocardiac junction. Chirurg 2011; 82: 447-449. doi: 10.1007/ s00104-010-1986-3 14. Crighton E, Botha A. Intraductal papillary mucinous neoplasm of the oesophagus: an unusual case of dysphagia. Ann R Coll Surg Engl 2012; 94: e92-e94. doi: 10.1308/003588412X13171221589090 15. Lowry DM, Mack TE, Partridge BJ, Barbick BC, Marks RM, Kindelan JT. Thorascopic resection of esophageal heterotopic pancreas. Ann Thorac Surg 2013; 96: 1850-1851. doi: 10.1016/j.athoracsur.2013.02.061 16. Filip R, Walczak E, Huk J, Radzki RP, Bieńko M. Heterotopic pancreatic tissue in the gastric cardia: a case report and literature review. World J Gastroenterol 2014; 20: 16779-16781. doi: 10.3748/wjg.v20.i44.16779 17. St Romain P, Muehlebach G, Damjanov I, Fan F. Adenocarcinoma arising in an ectopic mediastinal pancreas. Ann Diagn Pathol 2012; 16: 494-497. doi: 10.1016/j.anndiagpath.2011.04.005 18. Yan ML, Wang YD, Tian YF, Lin Y. Adenocarcinoma arising from intrahepatic heterotopic pancreas: a case report and literature review. World J Gastroenterol 2012; 18: 2881-2884. doi: 10.3748/wjg.v18. i22.2881 19. Okasha HH, Al-Bassiouni F, El-Ela MA, Al-Gemeie EH, Ezzat R. A retroperitoneal neuroendocrine tumor in ectopic pancreatic tissue. Endosc Ultrasound 2013; 2: 168-170. doi: 10.7178/eus.06.0012 20. Goodarzi M, Rashid A, Maru D. Invasive ductal adenocarcinoma arising from pancreatic heterotopia in rectum: case report and review of literature. Hum Pathol 2010; 41: 1809-1813. doi: 10.1016/j. humpath.2010.06.005 21. Jiang LX, Xu J, Wang XW, et al. Gastric outlet obstruction caused by heterotopic pancreas: A case report and a quick review. World J Gastroenterol 2008; 14: 6757-6759. doi: 10.3748/wjg.14.6757